
RSS-Feed abonnieren
DOI: 10.1055/s-0042-1744415
Survey of Areas Underserved by Plastic Surgery in Japan
Abstract
Background In Japan, there is a large regional disparity in plastic surgery availability. In order for plastic surgery to be widely available for all citizens, it is essential for at least one plastic surgery facility to be located in each secondary medical zone.
Methods Using the Japan Society of Plastic and Reconstructive Surgery homepage and some databases, we extracted data on secondary medical zones that do not have a plastic surgery facility. The national and regional coverage rates were calculated. The coverage rate for each group divided by the degree of population concentration was also calculated.
Results We found that 147 of 344 secondary medical zones did not have a plastic surgery facility, and the area coverage rate was found to be 57.27% nationwide. The coverage rate in terms of population was 87.07% (correlation coefficient of area and population coverage = 0.983). The area coverage rates in Hokkaido-Tohoku, Kanto, Chubu, Kansai, Chugoku-Shikoku, and Kyushu-Okinawa districts were 47.46, 72.15, 76.47, 62.79, 52.08, and 32.81%, respectively. The corresponding population coverage rates were 79.92, 91.62, 94.27, 90.59, 80.68, and 69.54%, respectively. The area coverage rates in metropolitan areas, provincial cities, and rural areas were 98.08, 75.90, and 15.87%, respectively. In contrast, the area coverage rate of dermatology was 62.79% and that of orthopaedics was 97.09%.
Conclusion Unfortunately, it is estimated that more than 40% of secondary medical zones are underserved by plastic surgery, and 13% of the population is not able to fully benefit from this specialty in Japan.
#
Japan promotes a national policy of “region-completed medical care” that seeks to differentiate and coordinate medical functions and provide continuous medical care throughout the acute, recovery, and long-term care periods. Each prefecture formulates its own medical plan according to the local circumstances, in which “medical zones” are defined as the regional units providing various services.
The most important “secondary medical zone” is a unit providing general health care, including health promotion, disease prevention, and hospital treatment, with the aim to complete services in that integrated area. Unlike tertiary medical zones, which aim to provide advanced or specialized care, the establishment of secondary medical zones must take into account the social environment, including natural conditions, traffic conditions, and supply–demand characteristics. Therefore, the suitability of the setting is directly linked to the quality of life of local residents.[1]
Each medical specialty listed in the formally-specified 19 basic fields should be considered in the infrastructure put in place for residents to enjoy a healthy and cultural life, as guaranteed by the constitution of Japan. To ensure that the benefits reach the residents, there must be at least one facility in each secondary medical zone that can provide specialized treatments. However, there are large regional disparities in the availability of plastic surgery, which can play an important role in the life of local residents.[2]
These disparities among different secondary medical zones pose certain questions, such as whether there are any secondary medical zones with no approved facilities, how many such zones (if any) exist, and whether there are differences according to districts. Few studies have been able to answer these questions. This study seeks to provide meaningful information to support the planning of appropriate allocation of medical resources in the future.
Methods
The certified facilities listed on the Japan Society of Plastic and Reconstructive Surgery's Web site[3] as of November 2019 were included in our evaluation regardless of the certification type. The information regarding the locations of these certified facilities was matched with the secondary medical zone database version 9.2.1_pro (https://www.wellness.co.jp/siteoperation/msd/) provided by Wellness Co., Ltd. (Tokyo, Japan). We then examined the number of certified facilities for plastic surgery in each of the 344 secondary medical zones nationwide.
The number of secondary medical zones with one or more certified facilities in each district of Japan, including Hokkaido-Tohoku, Kanto, Chubu, Kansai, Chugoku-Shikoku, and Kyushu-Okinawa, was divided by the total number of secondary medical zones in that district to calculate the area coverage rate of plastic surgery. In addition, the ratio of the total population of municipalities in the secondary medical zone where one or more certified facilities existed to the total population of each district was calculated as the population coverage rate.
Furthermore, according to the classification proposed by Takahashi,[4] we divided secondary medical zones into three groups depending on the degree of population concentration: metropolitan areas (population density ≥2,000 people/km2 or 1 million people), provincial cities (population density ≥200/km2 and ≥100,000 people, or population ≥200,000), and rural areas (the former two conditions not applicable). The coverage of each group was calculated.
For comparison, data on accredited training facilities from the Web site of the Japanese Dermatological Association[5] and the data on accredited facilities from the Web site of the Japan Orthopedic Association[6] were extracted and the coverage ratios were calculated similarly.
#
Results
There were a total of 523 certified plastic surgery facilities in Japan, and 147 secondary medical zones nationwide without any accredited institutions. The area coverage rate was only 57.27% (197/344), whereas the population coverage rate was 87.07%. The distribution of secondary medical zones according to the number of facilities is shown in [Fig. 1].

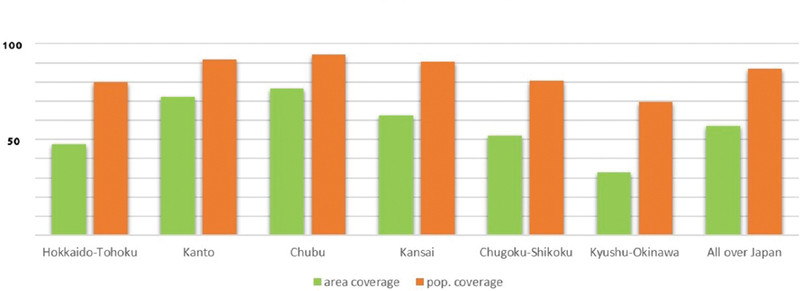
The area coverage rates in Hokkaido-Tohoku, Kanto, Chubu, Kansai, Chugoku-Shikoku, and Kyushu-Okinawa were 47.46% (28/59), 72.15% (57/79), 76.47% (39/51), 62.79% (27/43), 52.08% (25/48), and 32.81% (21/64), respectively. The corresponding population coverage rates were 79.92, 91.62, 94.27, 90.59, 80.68, and 69.54%, respectively ([Figs. 2]-[4]). A strong positive correlation was found between the area and population coverage rates in each district (r = 0.983, p < 0.01).


The area coverage rates in the metropolitan areas, provincial cities, and rural areas were 98.08% (51/52), 75.90% (126/166), and 15.87% (20/126), respectively ([Fig. 5]).

There were 649 dermatology facilities and 2,009 orthopedic facilities nationwide.
The nationwide area coverage rate of dermatology facilities was 62.79% (216/344) and the corresponding population coverage rate was 87.36%. The area coverage rates by district were 44.07, 73.42, 80.39, 86.05, 54.17, and 43.75%, respectively, in Hokkaido-Tohoku, Kanto, Chubu, Kansai, Chugoku-Shikoku, and Kyushu-Okinawa. The districts with a large disparity between the coverage of plastic surgery facilities and dermatology facilities were Kansai (over 20%) and Kyushu-Okinawa (over 10%).
The nationwide area coverage rate of orthopedic facilities was 97.09% (334/344), and the corresponding population coverage rate was 99.57%. The area coverage rates by district were 96.61, 98.73, 96.08, 100, 95.83, and 95.31%, respectively, in Hokkaido-Tohoku, Kanto, Chubu, Kansai, Chugoku-Shikoku, and Kyushu-Okinawa. A high coverage rate of over 95% was observed in all districts ([Fig. 6]).

#
Discussion
The results showed an alarming absence of certified facilities for plastic surgery in more than 40% of secondary medical zones. Although the population coverage rate was ∼87%, the study showed that ∼13% of the Japanese population lives in underserved areas where plastic surgery is not available.
It has been pointed out previously that tertiary medical zones are too large, which makes it challenging for residents of marginal areas to receive advanced treatments.[7] However, the focus of this study is not such rare cases (most people will only have the opportunity to receive such treatments at most once in their lives). The problem currently being tackled is whether standard treatment can be received on a regular basis, which is considered to be a more serious issue.
A counterargument exists that the practice of plastic surgery is often replaced by that of other specialties (e.g., general surgery, dermatology, and orthopaedics). The short history of plastic surgery in Japan is also evidence of the similar roles played by other practices since ancient times. Therefore, the improvement of plastic surgery is, unfortunately, relegated to a low priority among the basic medical fields.
However, there is a trend for each medical specialty to become increasingly specialized in its own field. Several common diseases, including those of the skin, exclusively require plastic surgery as treatment, which can be performed specifically by plastic surgeons (many dermatologists tend to avoid surgery).
Emphasizing only the cosmetic aspect of plastic surgery and regarding it as a representative of unessential and nonurgent care can lead to a lack of proper treatment for common diseases among residents in areas without plastic surgery facilities, placing them at greater risk.
As reflected by the phrase “disparities in health result from decisions made by society,”[8] responsibility for poor health should not be attributed solely to individuals. The fair distribution of medical resources should be considered our social responsibility. Although in many countries, these problems are often accompanied by complex social aspects such as racial disparities,[9] the situation in Japan is relatively simple and can be dealt with easily.
The Kanto, Chubu, and Kansai districts were found to have relatively high coverage rates, with 90% or more on a population basis. However, northern and southwestern Japan are in a grievous situation.
Several blank zones are noticeable in [Fig. 1]. In particular, about 70% of Kyushu can be classified as an underserved area, with 30% of the Kyushu population lacking access to plastic surgery, which highlights a concerning disparity.
Similarly, the disparity between urban areas and rural areas is also critical. The metropolitan areas had a coverage rate of 98%, including almost all medical zones, whereas the rural areas had a coverage rate of only 15%. Most people living in rural areas probably either abandon the opportunity to receive plastic surgery treatment on a regular basis or are unaware of its existence.
Here, we should consider the reasons for the substantial regional disparities identified in this study. Low awareness of plastic surgery may largely account for these disparities, possibly due to the brief history of plastic surgery. The scope of plastic surgery and its raison d'être are not widely known to the public.[2] Especially in outlying areas, there may be a lack of calls from local communities to launch facilities for plastic surgery.
In addition, postgraduate training hospitals are concentrated in cities; therefore, trainees do not gather in rural areas, which may promote disparities. This is also the case in France[10] and in other countries.
Nonetheless, a universal health care system has been fully implemented in Japan and citizens can benefit from most plastic surgery treatments at a small cost. Therefore, it is unlikely that the difference in regional economic power is related to the distribution of facilities.
Furthermore, the motivations of service providers also need to be examined. Considering the profitability of medical institutions, it is natural that there will be more facilities in areas with high populations. However, the purple areas shown in [Fig. 1] indicate disordered or overcrowded states of facilities. An excessive concentration of plastic surgery facilities will lead to enhanced competition with a consequent deterioration of profits.
It is noteworthy that there is no certified facility in one-fourth of the provincial city zones. The frontier for expansion is not limited to rural areas, but also includes local cities and suburbs with moderate populations.
While creating new facilities in the future, it is advisable to first expand into these provincial city areas to balance the local demand. This will benefit both the providers and recipients of medical care.
How can we ensure an even spread of plastic surgery services, from a broader perspective? Would this require government involvement or leadership from groups such as the Japan Society of Plastic and Reconstructive Surgery?
The urban “ceiling” system (setting an upper limit on the number of senior residents who can be trained in metropolitan areas) has already been put in place. Moreover, related laws and regulations have been amended in recent years. The transfer of medical administration authority from the central government to the prefectural governors and the provision of incentives for doctors working in poorly serviced areas are under consideration. Through these measures, we are attempting to eliminate the uneven distribution of medical services.
There are some policy examples overseas that we should refer to.[10] In Germany, each region has a maximum threshold for the number of doctors in each specialty. This is a mechanism to control regional disparities by limiting the opening of new medical practices. In one state in Canada, medical fees are being increased for doctors working in rural areas. Similarly, there are systems in the United States that give preferential treatment to medical students from sparsely populated areas, and tax reduction measures and subsidies when opening facilities in remote areas.
With the recent coronavirus disease 2019 pandemic, the introduction of telemedicine has gained momentum in our society.[11] Medical care in rural areas can certainly be replaced or supplemented to some extent by online facilities.
However, internal medicine, which focuses on diagnosis or medication, and plastic surgery are quite different. It is impossible to suture wounds, perform open drainage, or remove necrotic tissue online. Telesurgery is not expected to be accomplished in the near future—even robotic blood sampling has not yet been achieved.
Although remote technology may be useful as a tool for consultation and diagnostic imaging among doctors and between doctors and nurses, as a platform that is in a relatively early stage in our field, it will take a little longer for plastic surgery patients to truly benefit from telemedicine. The importance of the presence of local facilities will not diminish for the time being.
Comparisons with other specialties are critical to confirm the position of plastic surgery.
The number of dermatological facilities is ∼20% more than that of plastic surgery facilities, and the area coverage rate is almost 6% higher. Although there is almost no difference in terms of overall population coverage, there is a vast difference in area coverage in certain districts, especially the Kansai district.
It is noteworthy that dermatology has strong components of internal medicine; therefore, it is possible to take appropriate measures for most cases at individual clinics even if they are not certified. Hence, it may be unreasonable to compare the availability of medical care based on only the existence of certified facilities. This is a limitation of this study that should be considered in future research.
There are more than 2,000 accredited orthopaedic facilities nationwide, which is more than three times the number of plastic surgery facilities. Remarkably, orthopaedic facilities cover 97% of secondary medical zones, although a direct comparison to plastic surgery facilities is unreasonable due to the difference in the number of facilities.
In addition, a coverage rate of 95% or more in all districts indicates that facilities for orthopaedic surgery are widespread throughout the country. Even island and mountain areas have at least one facility ([Fig. 7]). The fact that the development of plastic surgery facilities is far behind must be taken seriously, regardless of factors such as the history and scale of the Japan Society of Plastic and Reconstructive Surgery.

It is estimated that more than 40% of secondary medical zones are underserved in Japan, and 13% of Japanese people are not able to benefit fully from plastic surgery. Severe disparities were also found between cities and countryside areas. Compared with other specialties such as orthopaedics, the disparities in availability were quite conspicuous.
It is important to bridge this gap in the future by improving accessibility and allocating medical resources appropriately.
We want plastic surgeons to know that there are still frontiers in our country. At the same time, we hope that residents of these areas will become more aware of plastic surgery.
#
#
Conflict of Interest
None declared.
Acknowledgments
The advice and support given by Prof. T. Takahashi (International University of Health and Welfare Graduate School) and T. Watanabe (Wellness Co., Ltd.) have been of great help in this study.
Prior Presentation
This study was presented at the 63rd Annual Meeting of the Japan Society of Plastic and Reconstructive Surgery: International Session, August 26–28, 2020, Nagoya, Japan.
-
References
- 1 Satoh E, Kumakawa T. Establishing medical care zone from residents perspectives: The accessibility of critical care in Kanagawa prefecture and Iwate prefecture as case studies. Hoken Iryou Kagaku 2013; 62: 46-51
- 2 Sato M. Regional disparity in plastic surgery availability in Japan: visualization of the permeation for residents. Jpn J Plast Surg 2019; 62: 539-546
- 3 The list of certified facilities by Japan Society of Plastic and Reconstructive Surgery. Available at: https://jsprs.or.jp/specialist/shutoku/current_seido/nintei_shisetsu_list/index.html
- 4 Working Paper No. 443 of Japan Medical Association Research Institute. Available at: https://www.jmari.med.or.jp/research/working/wr_697.html
- 5 Japanese Dermatological Association's accredited training facilities (as of March 6, 2020). Available at: https://www.dermatol.or.jp/modules/specialist/index.php?content_id=25
- 6 Accredited facility's list of Japan Orthopedic Association. Accessed June 18, 2020 at: https://www.joa.or.jp/joaSecretariats/public-hp/facility-search
- 7 Miwa M, Kawaguchi H, Arima H, Kawahara K. The effect of the development of an emergency transfer system on the travel time to tertiary care centres in Japan. Int J Health Geogr 2006; 5: 25
- 8 Woodward A, Kawachi I. Why should physicians be concerned about health inequalities? Because inequalities are unfair and hurt everyone. West J Med 2001; 175 (01) 6-7
- 9 Butler PD, Britt LD, Longaker MT. Ethnic diversity remains scarce in academic plastic and reconstructive surgery. Plast Reconstr Surg 2009; 123 (05) 1618-1627
- 10 Okochi J. The medical manpower policies in advanced countries: an international comparative study of measures to adjust the number of physicians based on their specialties or regions they serve. The Journal of Japan Society for Clinical Anesthesia 2005; 25: 467-472
- 11 Contreras CM, Metzger GA, Beane JD, Dedhia PH, Ejaz A, Pawlik TM. Telemedicine: Patient-provider clinical engagement during the COVID-19 pandemic and beyond. J Gastrointest Surg 2020; 24 (07) 1692-1697
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
06. April 2022
© 2022. The Korean Society of Plastic and Reconstructive Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Satoh E, Kumakawa T. Establishing medical care zone from residents perspectives: The accessibility of critical care in Kanagawa prefecture and Iwate prefecture as case studies. Hoken Iryou Kagaku 2013; 62: 46-51
- 2 Sato M. Regional disparity in plastic surgery availability in Japan: visualization of the permeation for residents. Jpn J Plast Surg 2019; 62: 539-546
- 3 The list of certified facilities by Japan Society of Plastic and Reconstructive Surgery. Available at: https://jsprs.or.jp/specialist/shutoku/current_seido/nintei_shisetsu_list/index.html
- 4 Working Paper No. 443 of Japan Medical Association Research Institute. Available at: https://www.jmari.med.or.jp/research/working/wr_697.html
- 5 Japanese Dermatological Association's accredited training facilities (as of March 6, 2020). Available at: https://www.dermatol.or.jp/modules/specialist/index.php?content_id=25
- 6 Accredited facility's list of Japan Orthopedic Association. Accessed June 18, 2020 at: https://www.joa.or.jp/joaSecretariats/public-hp/facility-search
- 7 Miwa M, Kawaguchi H, Arima H, Kawahara K. The effect of the development of an emergency transfer system on the travel time to tertiary care centres in Japan. Int J Health Geogr 2006; 5: 25
- 8 Woodward A, Kawachi I. Why should physicians be concerned about health inequalities? Because inequalities are unfair and hurt everyone. West J Med 2001; 175 (01) 6-7
- 9 Butler PD, Britt LD, Longaker MT. Ethnic diversity remains scarce in academic plastic and reconstructive surgery. Plast Reconstr Surg 2009; 123 (05) 1618-1627
- 10 Okochi J. The medical manpower policies in advanced countries: an international comparative study of measures to adjust the number of physicians based on their specialties or regions they serve. The Journal of Japan Society for Clinical Anesthesia 2005; 25: 467-472
- 11 Contreras CM, Metzger GA, Beane JD, Dedhia PH, Ejaz A, Pawlik TM. Telemedicine: Patient-provider clinical engagement during the COVID-19 pandemic and beyond. J Gastrointest Surg 2020; 24 (07) 1692-1697