

Subscribe to RSS
DOI: 10.1055/s-0042-1750384
Intratumoral and Peritumoral Brain Abscess Concomitant with Glioblastoma: Report of Two Cases with Review of Literature
Authors
Funding None.

Abstract
Intracranial abscess coexistent with a high grade glioma, without prior surgical intervention, is an unusual occurrence. This paper presents two such cases with Nocardia farcinica abscess surrounding the glioblastoma in an immunocompromised individual and Enterococcus faecium abscess within the glioblastoma in an immunocompetent patient. Adjuvant therapy was tapered as per each patient's clinical response. Till date, only eight cases of coexistent high-grade glioma and brain abscess have been reported in literature. This report stands distinct in highlighting the need to radiologically evaluate each foci of a multicentric cranial lesion on its own merit.
Introduction
Intracerebral abscess associated with glial neoplasm is an infrequent clinical presentation. Sellar or parasellar tumors may be complicated with intracerebral abscess due to the direct migration of microorganisms from the paranasal sinuses. However, bacteremia via hematogenous spread is an unusual course of event complicating an existing glioma within the brain. The first case of abscess associated with a glioma was reported by Noguerado et al in 1987.[1] Prior to this case, there were reports of abscess in association with pituitary adenoma, craniopharyngioma, and metastasis.[2] [3] [4] Subsequently, there have been abscess reported with existing meningiomas as well, probably due to the breached capillary endothelium leading to increased protein permeability.[5] We report two cases of concomitant brain abscess with glioblastoma (GBM) with abscess occurring peritumorally in one patient and intratumorally in the other patient along with reviewing the eight previous similar reports in literature.
Case Presentation
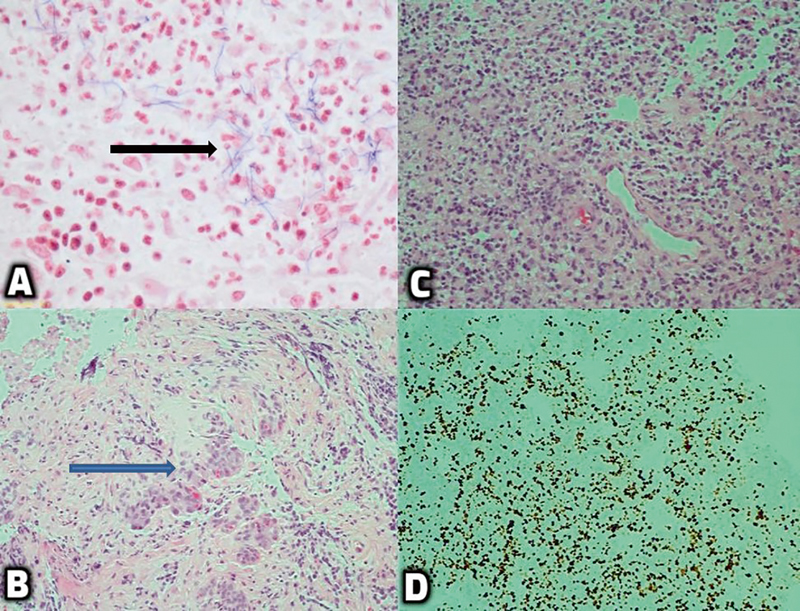
Case 1: A 65-year-old male, bricklayer by profession, was referred to our department with multiple seizures. He was already on antifungals for a month for lung aspergillosis. Magnetic resonance imaging (MRI) was suggestive of a solitary right posterior temporal lesion, showing T2 hyperintensity, mild diffusion restriction, and ring enhancement on contrast imaging ([Fig. 1]). Navigation sequence MRI performed within 3 weeks for surgical planning showed that radiologically there was marked change in the morphology of the lesion. There were now multiple cerebellar, frontal, and right temporal cystic lesions with marked central diffusion restriction overlying the earlier ring enhancing mass ([Fig. 2]). In view of the supporting history of lung aspergillosis, a provisional diagnosis of brain abscess was suspected, and excisional biopsy with debulking was performed of the cerebellar lesion. Pathology showed Gram-positive filamentous rod organism suggestive of a Nocardia farcinica abscess ([Fig. 3]). He was started on appropriate antibiotics. After initial clinical improvement, deterioration occurred within 6 weeks of his initial presentation. MRI showed resolution of the cerebellar abscess, but the temporal lesions persisted. A temporal surgery was performed which showed abscess superficially and a densely cellular glial tumor with pleomorphic astrocytic cells in the deeper component. Microvascular hyperplasia with Ki-67 score of 30% was diagnostic of a GBM. In view of his poor postoperative recovery (complicated by liver abscess and iliac vein thrombosis), prolonged need for antibiotics (3 months intravenous + 3 months oral) and unfavorable molecular profile (methyl guanine methyl transferase unmethylated and isocitrate dehydrogenase wild-type), he was advised palliative radiation (RT) (30 Gy in 6# after 6 weeks of diagnosis) while chemotherapy was withheld. Sadly, he passed away after 13 months of diagnosis.


Case 2: A 36-years-old gentleman with no morbidities presented to us with headaches, nausea, and vomiting for 7 days. Cranial imaging showed a mass in the left frontal lobe with marked edema and heterogeneous peripheral enhancement ([Fig. 4]). No extracranial lesion was detected on evaluation. As the inflammatory markers were within normal limits and the diffusion sequence did not show marked restriction, the multidisciplinary team (MDT) felt that the images were suggestive of high-grade glioma. Surgical intervention showed thick yellowish fluid in the core of the tumor which was aspirated and sent for analysis along with the bulk of the lesion. Microbiology culture showed Enterococcus faecium and histology was suggestive of an ATRX and p53 mutant GBM. He was advised antibiotics as per culture for 8 weeks after discussion with microbiologist. After the MDT discussion, it was decided to start him on adjuvant RT (60 Gy in 30#) after 4 weeks of antibiotics itself as he showed a good clinical recovery with settlement of inflammatory markers. Temozolomide (TMZ) was started after 6 weeks of antibiotics with concurrent RT for a month and on its own for five cycles after RT. He returned to work after 6 months of surgery. No tumor progression or abscess recurrence was seen on last follow-up of one and a half year after diagnosis.

Discussion
Intracranial infections are known to occur postoperatively after tumor excision. However, it is uncommon for them to occur together preceding any form of intervention. Initiating steroids may precipitate immunosuppression resulting in hematogenous spread from the extracranial foci to the brain. This abscess can then develop either within the tumor, adjacent to the tumor, or in a distant location as a separate space-occupying lesion. Abscess developing as collision lesions adjacent to a glial neoplasm, especially a high-grade glioma, may make it difficult to diagnose both the entities as distinct pathologies. They may mask the underlying pathology by masquerading as a single lesion with multifocal/multicentric spread. Another plausible hypothesis can be the presence of a hemorrhagic tumor, underlying infarct, or extensive perilesional edema. This disrupts the blood–brain barrier and may lead to provision of a conducive environment for the proliferation of microorganisms. Shankar et al[6] have reported the occurrence of brain abscess within a posterior fossa tumor secondary to ventriculoperitoneal shunt infection suggesting the role of foreign body insertion in their etiology as well. Tumors associated with extensive necrosis can also increase the chances of superimposed abscess owing to the localized oxygen depletion and resultant ischemia.
Staphylococcus aureus ([Table 1]) is the most common organism causing the abscess in high-grade gliomas. The routine risk factors do not differ from those which cause increased susceptibility to isolated brain abscess, that is, contiguous spread from adjacent structures, namely, paranasal sinus, dural sinus, nasopharynx, oral cavity, etc. Known extracranial infection foci leading to distant spread to the brain must be ruled out, namely cardiac valves, lung, etc.
|
Author/ Year |
Age/Sex |
Location of GBM |
Abscess organism |
Location of abscess |
Time of diagnosis |
Treatment |
Follow-up |
|---|---|---|---|---|---|---|---|
|
Noguerado et al 1987[1] |
78/M |
Occipital lobe |
Salmonella enteritidis |
Intratumoral |
Abscess diagnosed on CSF by LP. GBM diagnosed on autopsy |
Antibiotics |
Expired after 6 weeks of presentation |
|
Ichikawa et al 1992[11] |
46/F |
Frontal lobe |
Staphylococcus aureus |
Intratumoral |
Abscess diagnosed on radiology. GBM diagnosed on surgery after 5 months |
Antibiotics RT |
Expired after 13 months of presentation |
|
Sarria et al 2000[12] |
58/F |
Frontal lobe |
Salmonella enteritidis |
Intratumoral |
Abscess diagnosed on aspiration. GBM diagnosed on surgery after 6 weeks |
Antibiotics |
Expired after 52 days of presentation |
|
Kalita et al 2008[13] |
57/F |
Occipital lobe |
Staphylococcus aureus |
Intratumoral |
GBM suspected on radiology. GBM + abscess diagnosed on surgery |
Antibiotics RT after 3 weeks of surgery |
No recurrence at 4 months of follow-up |
|
Jho et al 2011[14] |
53/M |
Temporal lobe |
Staphylococcus, Acinetobacter Iwofii, Propionibacterium |
Intratumoral |
GBM suspected on radiology. GBM + abscess diagnosed on surgery |
Antibiotics. RT (6o Gy in 33#) after 4 weeks of surgery. 1 cycle TMZ after 12 weeks of surgery |
Recurrence at 4.5 months – Surgery + 3 cycles of TMZ. Recurrence at 8.5 months – 12 cycles of irinotecan and bevacizumab Recurrence at 19.5 months – 2 cycles of TMZ + bevacizumab for 3 weeks. Recurrence at 22 months – Erlotinib and Sirolimus. Expired after 2 years of presentation |
|
Tsugu et al 2012[15] |
45/M |
Temporal lobe |
Anaerobic Gram-negative bacilli |
Intratumoral |
GBM suspected on radiology. GBM + abscess diagnosed on surgery |
Antibiotics RT (66 Gy) + TMZ (120 mg/day) for 42 days after 4 weeks of surgery |
Recurrence at 5 months – Surgery + TMZ Recurrence at 14 months Expired after 22.5 months of presentation |
|
Singh et al 2013[16] |
50/M |
Fronto-parietal lobe |
Anaerobic gram-negative bacilli |
Intratumoral |
GBM suspected on radiology. GBM + abscess diagnosed on surgery |
Antibiotics RT (66 Gy) + TMZ (120 mg/day for 42 days) after 3 weeks of surgery |
Not mentioned |
|
Kishore et al 2018[17] |
45/F |
Frontal |
Enterococcus |
Intratumoral |
GBM or abscess suspected on radiology. GBM + abscess diagnosed on surgery |
Antibiotics RT + TMZ after 6 weeks of surgery |
No recurrence at 12 weeks |
|
Current case, 2021 |
65/M |
Temporal |
Nocardia farcinica |
Peritumoral |
Abscess suspected on radiology and confirmed on biopsy. GBM+ abscess diagnosed on second surgery after deep tissue analyzed |
Antibiotics Palliative RT (30 Gy in 6#) after 6 weeks of surgery TMZ withheld |
Expired after 13 months of diagnosis |
|
Current case, 2021 |
36/M |
Frontal |
Enterococcus faecium |
Intratumoral |
GBM suspected on radiology. GBM + abscess diagnosed on surgery |
Antibiotics RT (60 Gy in 30#) after 4 weeks of antibiotics TMZ after 6 weeks of antibiotics with concurrent RT for a month. 5 cycles of only TMZ |
No recurrence at 18 months of follow-up |
Abbreviations: CSF, cerebrospinal fluid; GBM, glioblastoma; LP, lumbar puncture; RT, radiation; TMZ, Temozolomide.
It is imperative to keep a high index of suspicion for the presence of two concomitant pathologies in multicentric lesions. MRI is the diagnostic investigation of choice.[7] [8] On computed tomography scan, both GBMs and abscess show a lesion having iso-/hyperdensity rim. They enhance on contrast administration and show central hypodensity with marked mass effect and vasogenic edema. Both show a fairly similar radiological profile on T1-weighted (hypo-/isointense GBM) and T2-weighted/fluid-attenuated inversion recovery (hyperintense) sequences of MRI. Diffusion-weighted sequences are imperative to achieve a more accurate radiological diagnosis. GBM show intermediate restriction while the central part of brain abscess shows marked restriction. Perfusion scans show that GBM are hyperperfused while abscess show reduced blood volume. On contrast imaging, GBM typically show thick, irregularly enhancing margins which can be multifocal. On the other hand, brain abscess has in its early encapsulation stage a thin enhancing rim with occasional additional multicentric “daughter” collections. Finally, on spectroscopy, voxels show peak of choline, lactate, and lipids with reduced N-acetyl aspartate in GBM, whereas abscess usually show elevated lipid lactate and amino acids peak. Recently, 99mTc-labeled LeukoScan has also been recommended to help in the diagnosis of infection with a high negative predictive value if performed prior to starting steroid therapy.[9]
In both our patients, we could not diagnose presence of glioma concurrent with abscess on radiology preoperatively. On retrospective evaluation, performing a spectroscopy MRI with voxels placed in the multicentric lesions and correlating it with perfusion and diffusion sequences would probably have helped us diagnose the presence of two different pathologies.
Surgery is the recommended mode of treatment which not only helps in diagnosis but also helps relieve the mass effect and reduce infective/tumor burden. The surgical team must be prepared to send culture specimens as well as formalin mounted pathology specimens to avoid missing the diagnosis. Although no protocol exists with regards to adjuvant therapy, the authors recommend tapering the regime based on individual patient's characteristics, that is, age, performance score, molecular status of the tumor, spread of the abscess, clinical and radiological response to antibiotics, etc. This may vary from as less as 4 weeks to as much as 12 weeks to being withheld completely.
Abscess associated with high-grade tumors can have a worse outcome due to the increased chances of rupture and subsequent meningitis or ventriculitis which can worsen the preexisting poor prognosis. Mortality rate in multiple Nocardia abscess can be as high as 66%.[10] Though a possible hypothesis exists of bacteria within the abscess showing preferential consumption of localized nutrients leading to delay in the progression of tumor,[11] this is yet to be corroborated by evidence-based research.
Among the eight similar reports documented in literature ([Table 1]),[1] [11] [12] [13] [14] [15] [16] [17] none of the cases were diagnosed as different entities on radiology presurgery. All but one case showed a solitary organism detected in the abscess. None of the previous cases show a peritumoral abscess with GBM, nor has a Nocardia farcinica abscess occurring together with GBM been reported earlier. The longest duration of follow-up mentioned is in a patient with multiorganism abscess along with temporal lobe GBM who expired after 2 years of follow-up. Adjuvant treatment regime in these cases included antibiotics only (2/8), antibiotics plus RT only (2/8), and antibiotics plus RT plus chemotherapy in the remaining 4 cases. RT was started after 3 weeks of surgery in 2 patients, after 4 weeks of surgery in 2 patients, and after 6 weeks of surgery in 1 patient. There was no mention of the timing of RT therapy in one case. TMZ was delayed till after 12 weeks of surgery in only one patient while in the remaining three patients who received it, TMZ was given along with the RT.
Conclusion
High-grade glioma presenting with a coexistent brain abscess is a very rare occurrence. The key challenge is to identify the two pathologies prior to surgery. Diffusion-weighted MRI, perfusion sequences and spectroscopy are essential to help make an early diagnosis. The authors recommend an individually tailored holistic approach in deciding to balance delayed or partial adjuvant oncological treatment with aggressive antimicrobial treatment. Documenting of cases with their follow-up outcomes will help in formulating appropriate guidelines with regards to adjuvant plan.
Conflict of Interest
All the authors declare that they have no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
-
References
- 1 Noguerado A, Cabanyes J, Vivancos J. et al. Abscess caused by Salmonella enteritidis within a glioblastoma multiforme. J Infect 1987; 15 (01) 61-63
- 2 Asenjo A. Absceso de neumococos operado en adonoma de transition de la hipifisis. Arch Soc Cir Chile 1950; 2: 312-314
- 3 Mohindra S, Gupta R, Mohindra S, Gupta SK, Radotra BD. Posterior-fossa intra-tumoural abscess: a report of three patients and literature review. Br J Neurosurg 2004; 18 (05) 556-560
- 4 Rodriguez RE, Valero V, Watanakunakorn C. Salmonella focal intracranial infections: review of the world literature (1884-1984) and report of an unusual case. Rev Infect Dis 1986; 8 (01) 31-41
- 5 Lo WB, Cahill J, Carey M, Mehta H, Shad A. Infected intracranial meningiomas. World Neurosurg 2014; 81 (3-4): 651.e9-651.e13
- 6 Shankar A, Chacko G, Chacko AG. Intratumoral abscess: an unusual complication of ventriculoperitoneal shunt infection. Childs Nerv Syst 2004; 20 (03) 204-206
- 7 Haimes AB, Zimmerman RD, Morgello S. et al. MR imaging of brain abscesses. AJR Am J Roentgenol 1989; 152 (05) 1073-1085
- 8 Lai PH, Ho JT, Chen WL. et al. Brain abscess and necrotic brain tumor: discrimination with proton MR spectroscopy and diffusion-weighted imaging. AJNR Am J Neuroradiol 2002; 23 (08) 1369-1377
- 9 Campennì A, Caruso G, Barresi V. et al. Gliomas with intratumoral abscess formation: Description of new cases, review of the literature, and the role of (99m)TC-LeukoScan. Kaohsiung J Med Sci 2015; 31 (07) 377-383
- 10 Lee GY, Daniel RT, Brophy BP, Reilly PL. Surgical treatment of nocardial brain abscesses. Neurosurgery 2002; 51 (03) 668-671 , discussion 671–672
- 11 Ichikawa M, Shimizu Y, Sato M. et al. Abscess within a glioblastoma multiforme–case report. Neurol Med Chir (Tokyo) 1992; 32 (11) 829-833
- 12 Sarria JC, Vidal AM, Kimbrough III RC. Salmonella enteritidis brain abscess: case report and review. Clin Neurol Neurosurg 2000; 102 (04) 236-239
- 13 Kalita O, Kala M, Svebisova H. et al. Glioblastoma multiforme with an abscess: case report and literature review. J Neurooncol 2008; 88 (02) 221-225
- 14 Jho DH, Spiliopoulos K, Stein TD, Williams Z. Concomitant presentation of a glioblastoma multiforme with superimposed abscess. World Neurosurg 2011; 75 (01) 126-131 , discussion 50–53
- 15 Tsugu A, Osada T, Nishiyama J, Matsumae M. Glioblastoma associated with intratumoral abscess formation. Case report. Neurol Med Chir (Tokyo) 2012; 52 (02) 99-102
- 16 Singh S, Singh S, Mohammad A, Hussain J. Unusual presentation of brain tumor with intratumoral abscess formation. Arch Int Surg 2013; 3: 66-69
- 17 Kishore K, Beniwal M, Rao S. et al. Abscess within a glioblastoma: mimicking a Matryoshka doll. World Neurosurg 2018; 113: 146-152
Address for correspondence
Publication History
Article published online:
25 August 2022
© 2022. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Noguerado A, Cabanyes J, Vivancos J. et al. Abscess caused by Salmonella enteritidis within a glioblastoma multiforme. J Infect 1987; 15 (01) 61-63
- 2 Asenjo A. Absceso de neumococos operado en adonoma de transition de la hipifisis. Arch Soc Cir Chile 1950; 2: 312-314
- 3 Mohindra S, Gupta R, Mohindra S, Gupta SK, Radotra BD. Posterior-fossa intra-tumoural abscess: a report of three patients and literature review. Br J Neurosurg 2004; 18 (05) 556-560
- 4 Rodriguez RE, Valero V, Watanakunakorn C. Salmonella focal intracranial infections: review of the world literature (1884-1984) and report of an unusual case. Rev Infect Dis 1986; 8 (01) 31-41
- 5 Lo WB, Cahill J, Carey M, Mehta H, Shad A. Infected intracranial meningiomas. World Neurosurg 2014; 81 (3-4): 651.e9-651.e13
- 6 Shankar A, Chacko G, Chacko AG. Intratumoral abscess: an unusual complication of ventriculoperitoneal shunt infection. Childs Nerv Syst 2004; 20 (03) 204-206
- 7 Haimes AB, Zimmerman RD, Morgello S. et al. MR imaging of brain abscesses. AJR Am J Roentgenol 1989; 152 (05) 1073-1085
- 8 Lai PH, Ho JT, Chen WL. et al. Brain abscess and necrotic brain tumor: discrimination with proton MR spectroscopy and diffusion-weighted imaging. AJNR Am J Neuroradiol 2002; 23 (08) 1369-1377
- 9 Campennì A, Caruso G, Barresi V. et al. Gliomas with intratumoral abscess formation: Description of new cases, review of the literature, and the role of (99m)TC-LeukoScan. Kaohsiung J Med Sci 2015; 31 (07) 377-383
- 10 Lee GY, Daniel RT, Brophy BP, Reilly PL. Surgical treatment of nocardial brain abscesses. Neurosurgery 2002; 51 (03) 668-671 , discussion 671–672
- 11 Ichikawa M, Shimizu Y, Sato M. et al. Abscess within a glioblastoma multiforme–case report. Neurol Med Chir (Tokyo) 1992; 32 (11) 829-833
- 12 Sarria JC, Vidal AM, Kimbrough III RC. Salmonella enteritidis brain abscess: case report and review. Clin Neurol Neurosurg 2000; 102 (04) 236-239
- 13 Kalita O, Kala M, Svebisova H. et al. Glioblastoma multiforme with an abscess: case report and literature review. J Neurooncol 2008; 88 (02) 221-225
- 14 Jho DH, Spiliopoulos K, Stein TD, Williams Z. Concomitant presentation of a glioblastoma multiforme with superimposed abscess. World Neurosurg 2011; 75 (01) 126-131 , discussion 50–53
- 15 Tsugu A, Osada T, Nishiyama J, Matsumae M. Glioblastoma associated with intratumoral abscess formation. Case report. Neurol Med Chir (Tokyo) 2012; 52 (02) 99-102
- 16 Singh S, Singh S, Mohammad A, Hussain J. Unusual presentation of brain tumor with intratumoral abscess formation. Arch Int Surg 2013; 3: 66-69
- 17 Kishore K, Beniwal M, Rao S. et al. Abscess within a glioblastoma: mimicking a Matryoshka doll. World Neurosurg 2018; 113: 146-152