

Subscribe to RSS
DOI: 10.1055/s-0043-1777847
Mycotic Pseudoaneurysm of the Internal Mammary Artery: An Unusual Complication of Tuberculosis—Managed with Percutaneous Glue Embolization
Authors


Abstract
Tuberculosis is still an endemic in many parts of the world. Vascular complications have been described in patients with tuberculosis and in aggressive chest infections such as actinomycoses. Etiology of internal mammary artery pseudoaneurysms includes iatrogenic causes or a complication of infection (mycotic aneurysm). Early diagnosis and treatment of these aneurysms are key to prevent complications such as hemorrhage, hemothorax, and hemorrhagic shock. In this case report, we describe the presentation and management of a 11-year-old patient with tuberculosis, who developed an internal mammary artery pseudoaneurysm during the course of treatment. We describe the case of a 11-year-old girl with known tuberculosis who developed a left internal mammary artery pseudoaneurysm, and treated with percutaneous ultrasound-guided glue embolization.
Introduction
Pulmonary tuberculosis (TB) can occasionally lead to vascular complications in the chest, involving both the pulmonary and bronchial vasculature. Mycotic pseudoaneurysm of internal mammary artery (IMA) is a sparsely reported vascular complication.[1] We herein report a rare case of IMA pseudoaneurysm due to the tubercular empyema in a child. IMA pseudoaneurysm commonly results from sternotomy, catheter insertion, central venous lines into subclavian vessels, or penetrating chest trauma such as stab injury. Very rarely the formation of an IMA pseudoaneurysm can be due to chest wall infection by staphylococcus, TB, or fungi. The potential risks of pseudoaneurysm of the IMA include late rupture, hemorrhage, exsanguinations, and death.[2]
Case Report
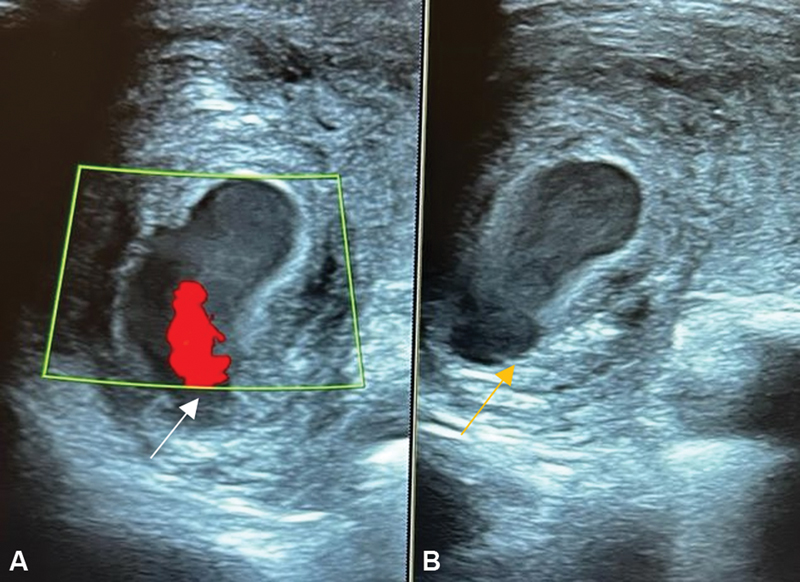
An 11-year-old girl with known TB complicated by pleural effusion, on first-line antitubercular drugs (isoniazid, rifampicin, pyrazinamide, and ethambutol), presented with gradual-onset swelling of the left anterior chest wall for the past 15 days. Physical examination revealed ill-defined soft tissue swelling involving the left chest measuring approximately 5 × 3 cm. Since the possibility of tubercular chest wall abscess was considered, aspiration was attempted under local anesthesia but only yielded blood. The child was then referred to radiology. Ultrasound (US) examination of the local site showed a rounded sac in close proximity to the IMA. The color Doppler showed a turbulent flow with the characteristic “yin-yang sign”- s/o pseudoaneurysm, having a narrow neck ([Fig. 1A] and [B]). This anterior chest wall lesion corresponded to a contrast-filled outpouching from the IMA on computed tomography (CT) angiography, surrounding hematoma seen underneath the chest wall predominantly in intermuscular planes, possibly secondary to needle aspiration ([Fig. 2A] and [B]). Associated significant finding included left empyema with necrotic mediastinal lymphadenopathy. Volume rendered three-dimensional (3D) reconstruction clearly showed a pseudoaneurysm from the IMA ([Fig. 3]).


The child underwent percutaneous US-guided glue embolization of the pseudoaneurysm, under sedation and local anesthesia. The immediate postprocedure US shows glue casting with complete obliteration of the pseudoaneurysm with no flow ([Fig. 4A–C]). The child also underwent a pleural biopsy using a Trucut needle that showed evidence of necrotizing granulomatous inflammation suggestive of TB. MGIT 960 TB cultures from the biopsy samples were negative. Patient was stable on follow-up with gradual reduction in the size of the swelling. US examination post 1 month of embolization showed no pseudoaneurysm ([Fig. 5]). The child was continued on antitubercular therapy with a total duration of 12 months. Pure glue was used in the procedure. It was injected directly into pseudoaneurysm sac; however, it did block the IMA by spillage. Since stenting across the neck was not possible due to unavailability of hardware for that small size. Reflux of glue into the parent vessel was inevitable as even if we would have deployed across the neck of pseudoaneurysm and in turn blocked the IMA. Also the IMA if blocked, there is collateralization of the ischemic area from inferior epigastric artery and intercostal arteries.


Result
-
1. The initial clinical examination suggested a swelling of 5 × 3 cm in size, with no thrill or bruit. However, after an attempted percutaneous aspiration, the CT angiogram revealed that the aneurysm was actually smaller, measuring 2.3 × 1.4 cm, and was surrounded by a hematoma.
Discussion
The IMA arises from the subclavian artery; it has collateral arteries to supply—anterior intercostal branches, distal part of the superior epigastric artery and musculophrenic artery. Because of its anatomic course, it is prone to injury by severe deceleration or penetrating injuries. Also, it is located within a vacuum-filled thoracic cavity and not surrounded by significant amounts of supporting tissue, in proximity to the dynamic motion of the chest wall, it is prone to get injured. These factors create a conducive environment for the development and possible rupture of an IMA pseudoaneurysm. Although nontraumatic IMA pseudoaneurysms are rare, a possible mechanism of development is the loss of elasticity resulting from structural vascular wall changes, such as those caused by cystic medial necrosis or hyperplasia.[3]
TB is a very common infectious disease, commonly caused by Mycobacterium tuberculosis through droplet infection. Tubercular infection in the chest can involve pulmonary as well as extrapulmonary portions, which include pleura, mediastinal structures, and chest wall.[4] Vascular complications involving the pulmonary and bronchial vessels are seen including arteritis and thrombosis, hypertrophy of the bronchial arteries, and Rasmussen aneurysm. These complications may result from direct involvement by M. tuberculosis of the vascular wall or as a consequence of contiguous spread from a TB mass.[5] M. tuberculosis can primarily involve the vessel wall in the area of active infection which may result in arteritis, thrombosis, or the pseudoaneurysm formation. Fibrin gradually replaces the granulation tissue that results in thinning of the arterial wall, pseudoaneurysm formation, and subsequent rupture. We believe that the same pathological process was the likely cause of the pseudoaneurysm formation in our index case.
The diagnosis of IMA pseudoaneurysm requires confirmation by chest CT angiography. Once an IMA pseudoaneurysm is diagnosed, determining the etiology of the disease is important: trauma, iatrogenic, fibromuscular dysplasia, polyarteritis nodosa, or infectious causes.
The general prognosis of IMA aneurysms is satisfactory. However, determining the appropriate treatment method for patients with vascular fragility is difficult.
In the past, symptomatic aneurysms were managed with conventional surgical repair (invasive approach associated with higher morbidity and mortality). However, due to recent developments in interventional radiology, varied treatment options such as US-guided compression, covered stent placement, coil embolization, and percutaneous embolization are available.
Cyanoacrylate glue (N-butyl 2 cyanoacrylate) is widely used as a visceral arterial embolic agent for endovascular treatment of intracranial vascular malformations and visceral pseudoaneurysms. Polymerization of monomers of cyanoacrylate and formation of a glue cast form the basis of use of this agent. This occurs instantaneously when the glue comes in contact with ions and free radicals present in body fluids. The main drawback of use of cyanoacrylate glue is the possibility of reflux of glue into the parent vessel. This can lead to nontarget embolization and ischemia of normal structures.[6]
Review of Literature
Vascular complications due to TB in chest involve the pulmonary as well as bronchial vasculature. Mycotic pseudoaneurysms of IMA are a sparsely reported clinical entity in the literature occurring due to TB. We report a rare case of IMA pseudoaneurysm due to the tubercular empyema in a patient with massive hemoptysis who was treated by endovascular coil embolization; however, the patient died due to refractory shock.[1]. In our index case, we report a similar entity, but we managed with percutaneous embolization and child is stable, doing well on follow-up.
Another case of pseudoaneurysm of the left IMA caused by pulmonary actinomycosis developed hemoptysis along with pain and swelling in the left upper chest wall. Multidetector CT with CT angiography showed a cavitating mass in the left upper lobe of the lung that infiltrated into the chest wall and a pseudoaneurysm of the left IMA. Imaging suggested that the lung mass resulted from pulmonary actinomycosis, which was confirmed by the histopathology of a fine-needle aspiration specimen.[2]. In our index case, the findings were similar although occurred as complication of TB.3
Conclusion
Pseudoaneurysm of the IMA is a possible differential in a patient with chest wall swelling in the presence of appropriate background risk factors. US with Doppler should be the first-line imaging modality to evaluate this swelling. Percutaneous glue embolization is an acceptable treatment option for the pseudoaneurysm of an IMA. TB should be addressed with the help of antituberculosis treatment.
Conflict of Interest
None declared.
-
References
- 1 Yadav MK, Bhatia A, Kumar S, Khandelwal N. Internal mammary artery pseudoaneurysm: a rare fatal complication of tubercular empyema. Lung India 2013; 30 (04) 341-343
- 2 Wani NA, Rawa IA, Pala NA, Kosar T. Pseudoaneurysm of internal mammary artery caused by pulmonary actinomycosis. Br J Radiol 2010; 83 (995) e235-e238
- 3 Prasad RM, Liu JZ, Garces C. et al. Uncommon cause of internal mammary artery pseudoaneurysm. Ochsner J 2022; 22 (03) 244-248
- 4 Kim HY, Song KS, Goo JM, Lee JS, Lee KS, Lim TH. Thoracic sequelae and complications of tuberculosis. Radiographics 2001; 21 (04) 839-858 , discussion 859–860
- 5 Deshmukh H, Prasad SR, Patankar T, Zankar M. Internal mammary artery pseudoaneurysms complicating chest wall infection in children: diagnosis and endovascular therapy. Clin Imaging 2001; 25 (06) 396-399
- 6 Mittal R, Stephen E, Keshava SN, Moses V, Agarwal S. Percutaneous cyanoacrylate glue embolization for peripheral pseudoaneurysms: an alternative treatment. Indian J Surg 2012; 74 (06) 483-485
Address for correspondence
Publication History
Article published online:
05 January 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Yadav MK, Bhatia A, Kumar S, Khandelwal N. Internal mammary artery pseudoaneurysm: a rare fatal complication of tubercular empyema. Lung India 2013; 30 (04) 341-343
- 2 Wani NA, Rawa IA, Pala NA, Kosar T. Pseudoaneurysm of internal mammary artery caused by pulmonary actinomycosis. Br J Radiol 2010; 83 (995) e235-e238
- 3 Prasad RM, Liu JZ, Garces C. et al. Uncommon cause of internal mammary artery pseudoaneurysm. Ochsner J 2022; 22 (03) 244-248
- 4 Kim HY, Song KS, Goo JM, Lee JS, Lee KS, Lim TH. Thoracic sequelae and complications of tuberculosis. Radiographics 2001; 21 (04) 839-858 , discussion 859–860
- 5 Deshmukh H, Prasad SR, Patankar T, Zankar M. Internal mammary artery pseudoaneurysms complicating chest wall infection in children: diagnosis and endovascular therapy. Clin Imaging 2001; 25 (06) 396-399
- 6 Mittal R, Stephen E, Keshava SN, Moses V, Agarwal S. Percutaneous cyanoacrylate glue embolization for peripheral pseudoaneurysms: an alternative treatment. Indian J Surg 2012; 74 (06) 483-485