

Subscribe to RSS
DOI: 10.1055/s-0044-1778727
Additional Role of 3D ASL Perfusion in Skull Base Lesions
Authors
Funding None.


Abstract
Background Arterial spin labeling (ASL) perfusion imaging is widely used since its main advantage is that no intravenous contrast is needed. Given that perfusion is a crucial biological characteristic for identifying tumor lesions, the qualitative noncontrast perfusion characteristics of these lesions were examined.
Aim We attempted utilizing the three-dimensional (3D) ASL technique to characterize skull base lesions and to highlight its crucial role in differentiating lesions.
Methods and Material 3D ASL imaging of 20 patients with posterior skull base lesions was performed in a 3-T magnetic resonance (MR) system (Siemens Healthineers, Skyra, Erlangen, Germany). The common differential diagnoses of skull base lesions could be distinguished based on this qualitative evaluation.
Results and Conclusions Glomus tumor has a strikingly increased perfusion when compared to meningiomas. The perfusion characteristics of metastasis depends on the primary tumor. Chondrosarcomas have a heterogeneously increased perfusion. Chordomas have variable perfusion, which helps in prognosticating the tumors. ASL benefits pediatric patients and in renal failure as well since it avoids the ethical ambiguity associated with contrast agents.
Introduction
Angiogenesis is a major factor in the growth of solid tumor lesions. Dynamic susceptibility contrast magnetic resonance imaging (DSC-MRI) is the gold standard method for analyzing angiogenesis. Even though conventional contrast-enhanced perfusion imaging is now a crucial component of the tumor investigation procedure, investigating extra-axial skull base lesions using this method is still difficult because of air–bone interface artifacts. The purpose of this study is to describe how three-dimensional (3D) arterial spin labeling (ASL) can characterize skull base lesions without the administration of contrast material. This method's significance keeps growing because it is noninvasive and enables the examination of patients with renal failure.
Materials and Methods
A cross-sectional study was conducted in which 20 patients with skull base lesions were studied. Informed written consent was acquired from every subject after explaining the details of this study. 3D ASL perfusion was done in addition to standard institute MRI protocol with added MR contrast sequences for certain cases in 3-T magnetic resonance scanner (Siemens Healthineers). Pre- and postcontrast fat-suppressed T1-weighted images and 3D magnetization prepared rapid gradient echo (MP RAGE) sequences were used for contrast imaging.
Extended ASL—continuous ASL (CASL) provides the largest ASL signal change, greatest signal-to-noise ratio (SNR), and can be advantageous.
Continuous labeling of the blood water is done during its passage through a label plane. Labeling is typically performed continuously for 1 to 2 seconds, after which a postlabeling delay is inserted before imaging. This delay allows the labeled blood to reach the region of interest in the brain and lets it clear from the feeding arteries.
The main disadvantage of ASL perfusion is the relatively longer acquisition time, resulting in potential motion artifacts.
Results
The 3D ASL technique is very helpful for identifying and differentiating skull base lesions by classifying the lesion's vascularity based on the qualitative evaluation. Meningiomas show increased perfusion when compared to schwannomas. The glomus tumors have a strikingly increased perfusion when compared to meningiomas. Chondrosarcomas have a heterogeneously increased perfusion. Chordomas have a variable perfusion that helps in prognosticating the tumors. The perfusion characteristics of metastasis depends on the primary tumor.
Discussion
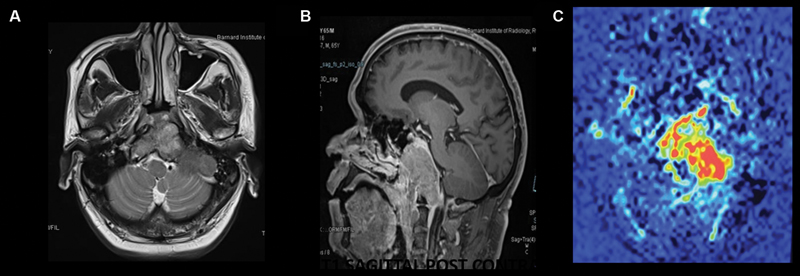
ASL imaging can be effectively used to distinguish between hypervascular and nonhypervascular lesions of the skull base by visually evaluating the characteristics of perfusion. We have highlighted cases at specific locations like the cerebellopontine angle cistern and Meckel's cave where meningiomas and schwannomas can be differentiated based on subjective perfusion evaluation. The qualitative characterization of the lesions allows for highly accurate diagnosis. An essential biological factor in the characterization of tumor lesions is perfusion evaluation.[1] While contrast enhancement makes it feasible to evaluate the blood–brain barrier disruption, perfusion patterns enable evaluation of the lesion's neoangiogenesis and microvascularization.[2] ASL was already used to assess the cerebral blood flow in cases of brain tumors, cerebrovascular abnormalities, and degenerative diseases.[3] Additionally, it was demonstrated to be a powerful replacement for the DSC-MRI technique and, more importantly, to provide more consistent blood flow measurement findings.[4] [5] ASL has a lower susceptibility to artifacts, so using it to image the base of the cranium can eliminate the issue with air–bone interface artefacts.[6] According to prior studies, the DSC-MRI technique could be used to distinguish between meningioma and schwannoma because the former has a more venous nature ([Figs. 1] [2] [3]). Studies of meningioma using ASL and DSC-MRI produced similar findings. When compared to meningiomas, ASL indicated that esthesioneuroblastomas had a comparatively less perfusion ([Figs. 4] and [5]). Further, chondrosarcomas of the sphenoid can occasionally be mistaken as a metastasis or chordoma based on morphological imaging. We think that ASL makes it simple to distinguish between the aforementioned kinds of lesions because metastasis ([Fig. 6]) and chordoma ([Figs. 7] and [8]) both exhibit variable perfusion, while chondrosarcomas exhibit a heterogeneously increased perfusion ([Fig. 9]). The ASL sequence is useful in predicting postoperative hemorrhage in pituitary adenoma in the pituitary region. Our results demonstrate that despite individual variations in adenoma perfusion, this tumor can be successfully differentiated from a meningioma by means of ASL since meningiomas are highly hyperperfused ([Figs. 10] and [11]), while adenomas are nonperfused or weakly perfused. However, based solely on the ASL pictures, we were unable to distinguish between a metastasis and a meningioma, since hypervascularity is encountered with few metastatic lesions, depending on the histologic type. Glomus tumors ([Fig. 12]) have a strikingly increased perfusion when compared to meningiomas. Additionally, even though the long-term effects of repetitive gadolinium-based contrast agent injections are debatable, contrast-free techniques are increasingly preferred.











The main limitations of this article are that only continuous ASL was used and so quantification could not be done and only limited numbers of lesions in each category were present ([Table 1]).
Abbreviations: ASL, arterial spin labeling; fs, fat-saturated.
Conclusion
Subjective evaluation of 3D ASL perfusion images yields information about perfusion characteristics in skull base tumors, which helps not only in highlighting the lesions like glomus tumors but also in differentiating other lesions like meningiomas from schwannomas. This pictorial depiction of the value of ASL perfusion stresses that 3D ASL perfusion when available can be a useful adjunct in the evaluation of skull base lesions and to differentiate between hypervascular and nonhypervascular lesions.
Conflict of Interest
None declared.
Acknowledgments
The author would like to thank the corresponding author, a beloved teacher and a mentor for his aid in completing this article.
Availability of Data and Material
The data are taken solely from our institution.
Authors' Contributions
J.F.N. did the major writeup of this case series. The majority of the cases in this review article were diagnosed by S.B.P. and followed up by J.F.N. The work was carried under the guidance of S.B.P. who provided us with insight and knowledge to diagnose indeterminate lesions with imaging alone.
-
References
- 1 Fujima N, Kudo K, Tsukahara A. et al. Measurement of tumor blood flow in head and neck squamous cell carcinoma by pseudo-continuous arterial spin labeling. Comparison With Dynamic Contrast-Enhanced MRI J Magn Reson Imaging 2015; 41: 983-991
- 2 Grade M, Hernandez Tamames JA, Pizzini FB, Achten E, Golay X, Smits M. A neuroradiologist's guide to arterial spin labeling MRI in clinical practice. Neuroradiology 2015; 57 (12) 1181-1202
- 3 Kimura H, Takeuchi H, Koshimoto Y. et al. Perfusion imaging of meningioma by using continuous arterial spin-labeling: comparison with dynamic susceptibility-weighted contrast-enhanced MR images and histopathologic features. Am J Neuroradiol 2006; 27 (01) 85-93
- 4 Jiang J, Zhao L, Zhang Y. et al. Comparative analysis of arterial spin labeling and dynamic susceptibility contrast perfusion imaging for quantitative perfusion measurements of brain tumors. Int J Clin Exp Pathol 2014; 7 (06) 2790-2799
- 5 Abe T, Mizobuchi Y, Sako W. et al. Clinical significance of discrepancy between arterial spin labeling images and contrast-enhanced images in the diagnosis of brain tumors. Magn Reson Med Sci 2015; 14 (04) 313-319
- 6 Haller S, Zaharchuk G, Thomas DL, Lovblad KO, Barkhof F, Golay X. Arterial spin labeling perfusion of the brain: emerging clinical applications. Radiology 2016; 281 (02) 337-356
Address for correspondence
Publication History
Article published online:
27 January 2024
© 2024. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Fujima N, Kudo K, Tsukahara A. et al. Measurement of tumor blood flow in head and neck squamous cell carcinoma by pseudo-continuous arterial spin labeling. Comparison With Dynamic Contrast-Enhanced MRI J Magn Reson Imaging 2015; 41: 983-991
- 2 Grade M, Hernandez Tamames JA, Pizzini FB, Achten E, Golay X, Smits M. A neuroradiologist's guide to arterial spin labeling MRI in clinical practice. Neuroradiology 2015; 57 (12) 1181-1202
- 3 Kimura H, Takeuchi H, Koshimoto Y. et al. Perfusion imaging of meningioma by using continuous arterial spin-labeling: comparison with dynamic susceptibility-weighted contrast-enhanced MR images and histopathologic features. Am J Neuroradiol 2006; 27 (01) 85-93
- 4 Jiang J, Zhao L, Zhang Y. et al. Comparative analysis of arterial spin labeling and dynamic susceptibility contrast perfusion imaging for quantitative perfusion measurements of brain tumors. Int J Clin Exp Pathol 2014; 7 (06) 2790-2799
- 5 Abe T, Mizobuchi Y, Sako W. et al. Clinical significance of discrepancy between arterial spin labeling images and contrast-enhanced images in the diagnosis of brain tumors. Magn Reson Med Sci 2015; 14 (04) 313-319
- 6 Haller S, Zaharchuk G, Thomas DL, Lovblad KO, Barkhof F, Golay X. Arterial spin labeling perfusion of the brain: emerging clinical applications. Radiology 2016; 281 (02) 337-356