

Subscribe to RSS
DOI: 10.12945/j.aorta.2017.16.015
Aorto-Cutaneous Fistula and False Aneurysm of the Ascending Aorta Five Years after its Prosthetic Replacement for Stanford Type A Acute Aortic Dissection
Authors
Corresponding Author
Publication History
09 June 2016
12 March 2017
Publication Date:
24 September 2018 (online)

Abstract
Aorto-cutaneous fistula and false aneurysm of the ascending aorta in patients who previously underwent Stanford Type A acute aortic dissection are rare and severe complications. Surgical correction remains a demanding challenge. In a case of false aneurysm rupture during redo sternotomy, selective cannulation of the right axillary and left carotid arteries allowed an efficient method of cerebral perfusion.
Introduction
False aneurysm (FA) occurring after replacement of the ascending aorta by a vascular prosthesis, which is defined as total or partial dehiscence of the prosthesis from the aortic wall, is a rare complication of this type of surgery. As with other aneurysms, it is notable for a marked increase in diameter and the occurrence of life-threatening complications such as rupture and fistula formation[1]. Despite advances in endovascular techniques, treatment in the majority of cases remains surgical. The procedure is complex, has a high mortality[2] [3], and represents a surgical challenge. Aorto-cutaneous fistula and FA of the ascending aorta is even more exceptional and challenging. The purpose of this case report is to describe our surgical strategy for aorto-cutaneous fistula associated with FA of the ascending aorta 5 years after its prosthetic replacement for Stanford Type A acute aortic dissection.
Case Presentation
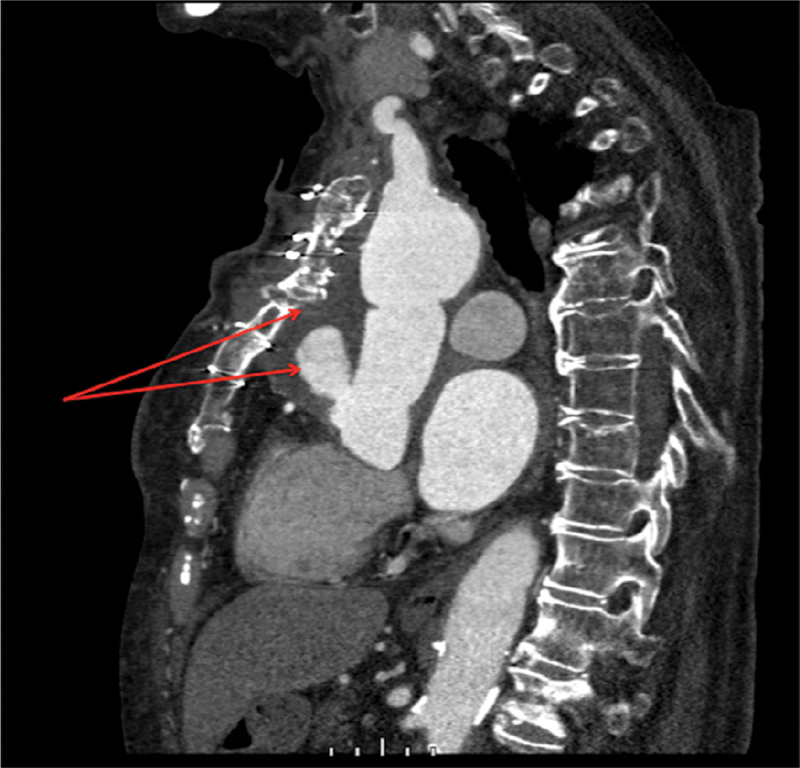
An 82-year-old woman underwent ascending aortic replacement in 2010 for a Stanford Type A acute aortic dissection. She remained well for Five years before exhibiting fresh, oozing blood from the upper part of the sternum ([Figure 1]). Computed chest tomography revealed anterior and posterior extensions of a FA of the ascending aorta with a communication with the skin through the sternum ([Figures 2], [3], and [4]).



Due to the risk of aortic rupture during sternotomy and the aortic dissection history, our surgical approach consisted of cannulating the right axillary and left carotid arteries through right axillary and left sternocleidomastoid cervical incisions by cardiopulmonary bypass (CPB) and cerebral protection for instituting hypothermic partial circulatory arrest before reentry into the chest. Cerebral protection was monitored with near-infrared spectroscopy. CPB and cooling were instituted before skin incision and stopped when the FA rupture occurred during the sternotomy. Cerebral protection was achieved by cooling the patient to 24°C, occluding the proximal left carotid and brachiocephalic arteries, and reducing bypass flow transiently to 800 mL/min. Mediastinal dissection and distal anastomosis between the hemi-arch and Dacron graft (Gelweave Vascutek Terumo, 32 mm) for hemi-arch replacement were performed under partial hypothermic circulatory arrest. The total duration of partial hypothermic circulatory arrest was 41 min. The distal Dacron graft was then cross-clamped, and normothermic full flow cardiopulmonary bypass (3900 mL/min) was restarted through the right axillary artery. Redo aortic root replacement (modified Bentall procedure) was performed using a biologic aortic valve (Trifecta, St. Jude Medical, 25 mm) and Dacron graft (Gelweave Vascutek Terumo, 28 mm). Finally, graft-to-graft anastomosis was performed. Distal and proximal graft anastomoses were performed using 4.0 monofilament running sutures at the aortic wall juncture and interrupted sutures at the annular level. Teflon reinforcement was used. Cross clamp duration was 80 min, and the total duration of CPB was 200 min. No intraoperative finding alluding to the etiology of the FA was identified. A diagnosis of prosthetic infection was excluded microbiologically. After debridement of the aorto-cutaneous fistula area, the sternum was rewired and the skin closed. The patient had an uncomplicated post-operative course and was transferred for cardiac rehabilitation 10 days after surgery.
Discussion
FA is a rare but serious and complex complication of ascending aorta and/or aortic root prosthetic replacement. Its incidence, risk factors, and natural history are unknown. Bachet et al.[4] reported three FAs in 143 patients initially undergoing operation for acute dissection of the ascending aorta with prosthetic replacement over a 10-year period. Also, Mohammadi et al. published the Pitie Salpetriere experience regarding 29 operations for FAs of the ascending aorta after prosthetic replacement, demonstrating that a well-planned operative strategy guided by preoperative imaging results in low operative mortality[5].
Major challenges of surgical therapy for these complex cases are choosing an approach that allows for safe reentry into the chest and efficient cerebral protection. The critical risk is FA rupture, which may lead to catastrophic hemorrhage during sternotomy. This risk is greater if the FA is situated retrosternally with an aorto-cutaneous fistula. Selective cerebral perfusion through the carotid arteries is the method of choice in our institution, and its efficacy for cerebral protection has been demonstrated[6] [7] [8]. This technique allows for mediastinal dissection and control of the distal aorta without compromising cerebral perfusion, even in cases of massive hemorrhage. In addition to its benefits in cases of FA rupture and exsanguination, this method allows for good operative exposure by positioning the carotid artery cannulas outside the operative field. This technique allows for unhurried mediastinal dissection and repair. In contrast to deep hypothermia, which requires long perfusion times for cooling and rewarming, a moderate level of hypothermia permits a shorter total bypass time, avoiding the disadvantages of deep hypothermia[5].
In conclusion, selective cannulation of the right axillary and left carotid arteries allowed an efficient method of cerebral perfusion and protection in this case of FA rupture during sternotomy. A well-planned operative strategy guided by preoperative imaging permitted careful analysis of the lesions, resulting in a good outcome for our patient.
Conflict of Interest
The authors have no conflicts of interest relevant to this publication.
† These authors contributed equally to this work
-
References
- 1 Mulder EJ, van Boeckel JH, Maas J, van den Akker PJ, Hermans J. Morbidity and mortality of reconstructive surgery of noninfected false aneurysms detected long after aortic prosthetic reconstruction. Arch Surg 1998; 133: 45-49 . DOI: 10.1001/archsurg.133.1.45
- 2 Razzouk A, Gundry S, Wang N, Heyner R, Sciolaro C, Van Arsdell G. , et al. Pseudoaneurysms of the aorta after cardiac surgery or chest trauma. Am Surg 1993; 59: 818-823 . PMID: 8256935
- 3 Sullivan K, Steiner R, Smullens S, Griska L, Meister S. Pseudoaneurysm of the ascending aorta following cardiac surgery. Chest 1988; 93: 138-143 . DOI: 10.1378/chest.93.1.138
- 4 Bachet JE, Termignon JL, Dreyfus G, Goudot B, Martinelli L, Piquois A. , et al. Aortic dissection prevalence, cause, and results of late reoperations. J Thorac Cardiovasc Surg 1994; 108: 199-205 . PMID: 8041167
- 5 Mohammadi S, Bonnet N, Leprince P, Kolsi M, Rama A, Pavie A. , et al. Reoperation for false aneurysm of the ascending aorta after its prosthetic replacement: surgical strategy. Ann Thorac Surg 2005; 79: 147-152 . DOI: 10.1016/j.athoracsur.2004.06.032
- 6 Sakurada T, Kazui T, Tanaka H, Komatsu S. Comparative experimental study of cerebral protection during aortic arch reconstruction. Ann Thorac Surg 1996; 61: 1348-1354 . DOI: 10.1016/0003-4975(96)00026-4
- 7 Kazui T, Kimura N, Yamada O, Komatsu S. Surgical outcome of aortic arch aneurysms using selective cerebral perfusion. Ann Thorac Surg 1994; 57: 904-911 . DOI: 10.1016/0003-4975(94)90201-1
- 8 Bachet J, Guilmet D. Brain protection during surgery of the aortic arch. J Card Surg 2002; 17: 115-124 . DOI: 10.1111/j.1540-8191.2002.tb01185.x
Corresponding Author
-
References
- 1 Mulder EJ, van Boeckel JH, Maas J, van den Akker PJ, Hermans J. Morbidity and mortality of reconstructive surgery of noninfected false aneurysms detected long after aortic prosthetic reconstruction. Arch Surg 1998; 133: 45-49 . DOI: 10.1001/archsurg.133.1.45
- 2 Razzouk A, Gundry S, Wang N, Heyner R, Sciolaro C, Van Arsdell G. , et al. Pseudoaneurysms of the aorta after cardiac surgery or chest trauma. Am Surg 1993; 59: 818-823 . PMID: 8256935
- 3 Sullivan K, Steiner R, Smullens S, Griska L, Meister S. Pseudoaneurysm of the ascending aorta following cardiac surgery. Chest 1988; 93: 138-143 . DOI: 10.1378/chest.93.1.138
- 4 Bachet JE, Termignon JL, Dreyfus G, Goudot B, Martinelli L, Piquois A. , et al. Aortic dissection prevalence, cause, and results of late reoperations. J Thorac Cardiovasc Surg 1994; 108: 199-205 . PMID: 8041167
- 5 Mohammadi S, Bonnet N, Leprince P, Kolsi M, Rama A, Pavie A. , et al. Reoperation for false aneurysm of the ascending aorta after its prosthetic replacement: surgical strategy. Ann Thorac Surg 2005; 79: 147-152 . DOI: 10.1016/j.athoracsur.2004.06.032
- 6 Sakurada T, Kazui T, Tanaka H, Komatsu S. Comparative experimental study of cerebral protection during aortic arch reconstruction. Ann Thorac Surg 1996; 61: 1348-1354 . DOI: 10.1016/0003-4975(96)00026-4
- 7 Kazui T, Kimura N, Yamada O, Komatsu S. Surgical outcome of aortic arch aneurysms using selective cerebral perfusion. Ann Thorac Surg 1994; 57: 904-911 . DOI: 10.1016/0003-4975(94)90201-1
- 8 Bachet J, Guilmet D. Brain protection during surgery of the aortic arch. J Card Surg 2002; 17: 115-124 . DOI: 10.1111/j.1540-8191.2002.tb01185.x