

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_266_17
Microvascular decompression in patients aged 30 years or younger
Authors

Objective: The aim of this study was to identify the etiology of hemifacial spasm (HFS) and trigeminal neuralgia (TN) in patients aged 30 years or younger and to examine the efficacy of microvascular decompression (MVD). Patients and Methods: Between 1996 and 2012, 228 HFS and 190 TN patients underwent MVD at Atsuchi Neurosurgical Hospital. Of these, 7 patients were 30 years of age or younger at the time of treatment (HFS: n = 6, TN: n = 1). Assessments were based on their medical history and on magnetic resonance imaging, magnetic resonance angiography, surgical, and follow-up findings. Results: The age of the 6 HFS patients ranged from 23 to 30 years (mean 27.8 ± 1.8 [standard deviation] years) at the time of surgery; the earliest symptom onset was in an 11-year-old boy. We noted vascular variations in 5 patients, a duplicate posterior inferior cerebellar artery in 2 patients, a short basilar artery in 1 patient, and an aberrant arterial course in 2 patients. At the latest follow-up, 1–69 months after MVD, 5 of the HFS patients were asymptomatic and the 6th had mild residual symptoms. A 23-year-old TN female underwent straightening of the trigeminal nerve by separation of a thickened arachnoid membrane from the nerve and dislocation of a small branch of the superior cerebellar artery from the distal end of the root exit zone. While she continued to experience occasional facial pain 48 months after the operation, she required no medication because surgery yielded significant pain amelioration. Conclusion: Although the pathogenesis of early-onset HFS and TN remains unclear, our findings suggest that vascular variations may be related to the etiology of vascular compression symptoms in patients with HFS or TN. MVD was useful for the treatment of neurovascular compression symptoms in young patients.
Introduction
Microvascular decompression (MVD) for hyperactive dysfunction of cranial nerves was developed by Gardner and Miklos [[1]],[[2]] and discussed by Jannetta [[3]],[[4]],[[5]] after the introduction of microsurgery under an operative microscope. MVD for trigeminal neuralgia (TN) has been shown to afford complete and long-lasting relief of pain in 70%–91% of adult patients.[[6]],[[7]] On hemifacial spasm (HFS), the cure rate of MVD was from 54% to 85%.[[8]],[[9]],[[10]],[[11]],[[12]] HFS is seen almost exclusively in middle-aged and older individuals, predominately women.[[3]],[[4]],[[5]],[[13]],[[14]] It is extremely rare in children.[[15]],[[16]],[[17]],[[18]] TN, primarily a disease of the elderly, is thought to be related to atherosclerotic changes in posterior fossa arteries that increase their tortuosity and result in the vascular compression that elicits TN.[[19]] Hemodynamic effects due to the aging process and to hypertension in elderly patients result in the elongation, redundancy, and atherosclerosis of the involved artery.[[3]],[[16]] Such changes in the vasculature are not likely to be implicated in younger patients with HFS and TN. We reviewed 6 patients with HFS and 1 patient with TN who underwent MVD at a single institution (contributor's institute no. 3) when they were 30 years old or younger.
Patients and Methods
Among 418 patients who underwent MVD between January 1996 and December 2012, 228 (55%) presented with HFS and 190 (45%) presented with TN; 142 HFS (62%) and 114 TN patients (60%) were female. HFS was on the left side in 126 of the 228 HFS patients (55%); TN was on the right side in 115 of the 190 TN patients (61%) [[Table 1]].

We focused on 7 patients who were 30 years old or younger at the time of MVD; 6 patients were treated for HFS and 1 patient for TN. The age of 30 years or younger accounted for 2.64% (6/227) of all HFS patients and 0.52% (1/190) of all TN patients. The patients underwent preoperative magnetic resonance imaging (MRI) studies including fast imaging with steady-state acquisition (FIESTA); in all patients, we acquired magnetic resonance angiography (MRA) images.
Surgical technique for microvascular decompression
All procedures were performed by exploring the cerebellopontine angle through a small retrosigmoid craniectomy; auditory brain stem evoked responses were monitored throughout the procedure. For HFS, we dissected the arachnoid membrane covering the 9th, 10th, and 11th cranial nerves for easy retraction of the flocculonodular lobe. After reaching the root exit zone (REZ) of the facial nerve, the involved artery was mobilized from the compressed facial nerve and an arterial loop was fixed to the dura with a bundle of Teflon fibers soaked in fibrin glue. For TN, the horizontal fissure of the cerebellum was opened widely to visualize the root entry zone (REZ) of the trigeminal nerve for identification of the involved vessel.
Ethical consideration
This retrospective study was approved by the Ethical Committee (reference no: 170159) at contributor's institute no. 2.
Results
Hemifacial spasm in youth
Neither 6 patients with HFS (4 males, 2 females, age range 23–30 years at the time of surgery, mean 27.8 + 1.8) nor a 23-year-old female patient with TN had a history of head injury, intracranial tumors, meningitis, or other infectious diseases [[Table 2]]. Different from the older HFS group (n=222) with 97 (44%) on the right side and 125 (56%) on the left side, 5 of 6 HFS patients younger than 30 years old were strongly involved on the right side. The earliest onset occurred at the age of 11 years (Case 1), and in the other 5 patients, the age at onset ranged from 23 to 30 years. One patient (Case 2) suffered persistent facial spasms for 2 years after her first MVD procedure performed at a different institute when he was 22 years old and mild spasms after undergoing MVD at our hospital. The initial symptom in 5 patients was a slight twitching of the lower eyelid, which later involved the entire face ipsilaterally. In 4 patients (Cases 1, 2, 3, and 6), we observed mild facial spasms at the time of discharge; at the latest postoperative follow-up (mean 29.7 months), 5 patients (Cases 2–6) were asymptomatic. None of the operated patients developed postoperative complications.

Vascular variations in hemifacial spasm
In Case 1, the anterior inferior cerebellar artery (AICA) was located between the distal part of the 7th and 8th cranial nerve [[Figure 1]]. Case 2 presented with a posterior inferior cerebellar artery (PICA) duplication [[Figure 2]]. MRI showed that the PICA of the distal origin compressed the REZ. The 4th patient also harbored a PICA duplication [[Figure 3]]; MRI revealed that the distal PICA was involved. In the 5th patient, the right AICA originated from the distal vertebral artery (VA). This patient's basilar artery (BA) was short (18 mm) [[Figure 4]]; its loop compressed the REZ. The AICA was transpositioned and fixed to dura mater. Intraoperatively, we detected no atherosclerotic changes in arteries explored during surgery in any of the 5 patients.




Trigeminal neuralgia in a youth
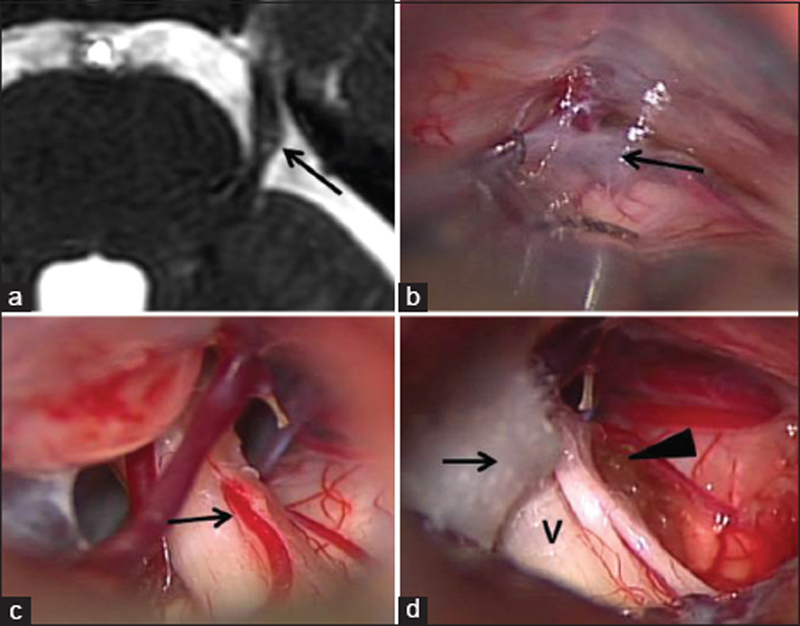
Our sole patient with left-sided TN (Case 7) was initially treated with carbamazepine, which yielded pain amelioration. However, her pain reappeared 4 weeks later and MRI revealed deformation of the trigeminal nerve root [[Figure 5]]. Intraoperatively, we found that a thick arachnoid membrane surrounded the trigeminal nerve. A branch of the left superior cerebellar artery (SCA) passed between the motor and sensory components of the nerve at the distal part of the REZ, and the root was bent dorsally. Separating the membrane from the nerve fibers straightened the trigeminal root. After separating a branch of the SCA from the nerve fibers, we transpositioned it distally from the REZ and fixed it to the dura mater with Teflon fibers and fibrin glue. In the course of 4-year postoperative follow-up, she reported occasional facial pain not requiring medication.
Discussion
Hemifacial spasms in youth
HFS is primarily seen in middle-aged and older individuals;[[3]],[[4]],[[5]],[[12]],[[19]] primary HFS is extremely rare in younger persons.[[15]],[[16]],[[17]],[[18]] The major offending vessel in 4 of our 6 young HFS patients was the PICA; the AICA was involved in the other 2 cases. In 5 previously reported HFS patients younger than 18 years, the major offender was the AICA.[[20]] In another series of individuals younger than 25 years, the PICA was involved in 17 (51.5%) and the AICA in 13 (39.4%) of 33 patients. Multiple vessels were implicated in the other 3 patients (9.1%).[[21]] Ehni and Woltman first suggested atherosclerosis as a possible etiology in patients with HFS [[15]] and Jannetta [[3]] cited elongation and tortuosity of the vascular loop and sagging of the brain that accompanies the aging process as factors in vascular compression in the elderly. Such vasculitic change of the offending vessels do not adequately explain HFS in young individuals. While arachnoid membrane thickening, venous compression, and venous anomalies may trigger HSF in some young individuals,[[16]],[[20]],[[22]],[[23]],[[24]] Chang et al.[[21]] detected neither anatomical vessel variations nor arachnoid thickening around the REZ and cerebellopontine cistern in their series. Others [[23]] attributed HFS to a posterior cranial fossa of small volume due to basilar invagination and/or a flat skull base [[23]] or to narrowing of the posterior fossa and a Chiari type 1 malformation resulting in the neurovascular compression seen in patients with HFS.[[25]],[[26]]
Trigeminal neuralgia in youth
Mason et al.[[27]] encountered a 13-month-old child with typical TN; the patient underwent MVD at the age of 7 years when marked venous compression of the nerve was revealed. In their large series, Resnick et al.[[28]] reported 23 patients in whom TN developed at an age younger than 18 years. Their patients underwent surgery at a mean age of 29.1 years, venous compression was found in 20 (87%). While Matsushima et al.[[29]] reported that TN due to venous compression is rare (5.8%), others documented a high rate in TN patients, including young individuals [[Table 3]].[[28]],[[30]],[[31]],[[32]]

Our series included one patient with TN (Case 7); it first occurred appeared when she was 23 years old. We detected no venous compression, rather, a thickened arachnoid membrane bent the trigeminal root, and the SCA branch went through the root, a phenomenon that has also been observed in patients with HFS.
Vascular variations
While Jho and Jannetta [[16]] suggested that anatomical variations in vessels at the base of the brain or at the REZ contribute to the development of HFS in youngsters,[[16]] Chang et al.[[21]] detected no such anatomic variations and no arachnoid thickening. In older patients, a characteristic angiographic finding is enlargement of the VA on the side ipsilateral to the HFS, resulting in a sharp, hairpin curve at the 4th segment of the VA. Furthermore, the ipsilateral PICA which branches at the angulated portion is commonly more ectatic, elongated, and redundant than the vessel on the contralateral side.[[33]] While vertebral angiograms of young HFS patients usually do not show such changes in the vasculature of the vertebro-BA,[[22]] 5 of our 7 patients manifested various types of vascular variations. Two patients (Cases 2 and 4) had a PICA duplication with the distal PICA being the offender; in another 2 (Cases 3 and 6), we detected an aberrant arterial course. The AICA ran between the 7th and 8th nerves in a patient with HFS (Case 1) and a branch of the SCA ran between the motor and sensory components of the 5th nerve in our TN patient (Case 7). The length of BA was reported to be 24–36 mm (average 30 mm).[[34]],[[35]] According to Saeki and Rhoton,[[36]] it ranges from 15 to 40 mm (mean 32 mm). Based on our MRA measurements, it ranged from 18.0 to 27.3 mm (mean 22.5 ± 2.7 mm) and we cannot preclude a length underestimation. In one patient with HFS (Case 5), the BA length was only 18 mm.
Vascular compression syndrome (HFS or TN) cannot be attributed to any particular type of variation because vascular variations are not very rare although we observed this phenomenon in 5 of our 7 patients. We think that vascular variations may be involved in the etiology of vascular compression syndrome in young adults. Ohta et al.[[37]] reported that arteriosclerotic changes were not involved in the pathogenesis of HFS and that vascular compression syndrome was attributable, even in adults, to anatomical features of the intracranial arteries and facial nerves formed during the prenatal stage.
Surgical outcome of microvascular decompression in young patients
Although mild facial spasms persisted in the perioperative period in 4 of our 6 HFS patients, in the course of postoperative follow-up (mean 29.71 months), 5 reported their complete disappearance. Samii et al.[[38]] found that among 117 HFS patients (mean age 54.5 years) who underwent MVD, 69 (59%) were spasm free at the time of discharge and 106 (91%) experienced no symptoms during a mean follow-up duration of 9.4 years. In another series of 1642 HFS patients, 56 (3.4%) of whom were younger than 30 years at the time of MVD; there was no significant difference between young and older patients in terms of symptom duration and surgical outcomes.[[39]] Therefore, immediate as well as long-term postoperative outcomes appear to be similar in young and older patients with HFS. Thickening of the arachnoid membrane (our Case 7) and a small posterior cranial fossa volume may not be predictive of a poor prognosis after MVD; while the prognosis may be poor in cases, the offending vessel is a vein [[Table 3]].[[20]],[[22]],[[23]]
In 294 of 362 adults (81%) with TN, Sindou et al.[[40]] reported a successful outcome 1 year after MVD; the cure rate fell to 75% at 15 years. Barker et al.[[7]] also obtained an excellent outcome (79.7%) at 1 year after surgery in their TN patients; the outcome at 10 years was also excellent in 69.6%. In other case series, MVD to treat TN in young patients yielded unsatisfactory results [[28]],[[30]],[[32]] although Bender et al.[[31]] reported a good outcome in 83% of their patients [[Table 3]]. TN associated with veins is more common in young patients and may be a factor associated with unfavorable MVD outcomes in young TN patients.
Conclusion
Although the etiology of early-onset HFS and TN remains unclear, our findings suggest that vascular variations may be a contributing factor in the nerve compression seen in younger patients. At least with respect to young HFS patients, the outcomes of MVD are comparable to those in older patients.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Gardner WJ, Miklos MV. Response of trigeminal neuralgia to decompression of sensory
root; discussion of cause of trigeminal neuralgia. J Am Med Assoc 1959;170:1773-6.
- 2 Gardner WJ, Sava GA. Hemifacial spasm: A reversible pathophysiologic state. J Neurosurg
1962;19:240-7.
- 3 Jannetta PJ. Neurovascular compression in cranial nerve and systemic disease. Ann
Surg 1980;192:518-25.
- 4 Jannetta PJ. Treatment of trigeminal neuralgia by microoperative decompression. In:
Youmans JR, editors. Neurological Surgery. 2nd ed. Vol. 6. Philadelphia, USA: W.B.
Saunders Co.; 1982. p. 3589-603.
- 5 Jannetta PJ. Microsurgical management of trigeminal neuralgia. Arch Neurol 1985;42:800.
- 6 Barba D, Alksne JF. Success of microvascular decompression with and without prior
surgical therapy for trigeminal neuralgia. J Neurosurg 1984;60:104-7.
- 7 Barker FG 2nd, Jannetta PJ, Bissonette DJ, Larkins MV, Jho HD. The long-term outcome
of microvascular decompression for trigeminal neuralgia. N Engl J Med 1996;334:1077-83.
- 8 Choi SJ, Sung KW, Sung WH, Lee JS, Kang JK, Choi CR. The clinical analysis of 75
patients which were operated on MVD. J Korean Neurosurg Soc 1990;19:506-12.
- 9 Huang CI, Chen IH, Lee LS. Microvascular decompression for hemifacial spasm: Analyses
of operative findings and results in 310 patients. Neurosurgery 1992;30:53-6.
- 10 Huh R, Han IB, Moon JY, Chang JW, Chung SS. Microvascular decompression for hemifacial
spasm: Analyses of operative complications in 1582 consecutive patients. Surg Neurol
2008;69:153-7.
- 11 Jang IH, Lee YH, Chung UW. Intraoperative electromyographic monitoring of the facial
nerve during microvascular decompression for hemifacial spasm. J Korean Acad Rehabil
Med 1994;18:142-51.
- 12 Jannetta PJ. Hemifacial spasm. Neurol Neurosurg Update Ser 1982;3:1-7.
- 13 Loeser JD, Chen J. Hemifacial spasm: Treatment by microsurgical facial nerve decompression.
Neurosurgery 1983;13:141-6.
- 14 Wilkins RH. Hemifacial spasm: A review. Surg Neurol 1991;36:251-77.
- 15 Ehni G, Woltman HW. Hemifacial spasm: Review of one hundred and six cases. Arch Neurol
Psychiatry 1945;53:205-11.
- 16 Jho HD, Jannetta PJ. Hemifacial spasm in young people treated with microvascular
decompression of the facial nerve. Neurosurgery 1987;20:767-70.
- 17 Langston JW, Tharp BR. Infantile hemifacial spasm. Arch Neurol 1976;33:302-3.
- 18 Milani N, Scaioli V, Giombini S, Grisoli M, Angelini L. Hemifacial spasm in a child.
Childs Nerv Syst 1991;7:466-8.
- 19 Jannetta PJ. Arterial compression of the trigeminal nerve at the pons in patients
with trigeminal neuralgia. J Neurosurg 1967;26 Suppl:159-62.
- 20 Feng B, Zheng X, Zhang W, Yang M, Tang Y, Zhong J, et al. Surgical treatment of pediatric
hemifacial spasm patients. Acta Neurochir (Wien) 2011;153:1031-5.
- 21 Chang JW, Chang JH, Park YG, Chung SS. Microvascular decompression of the facial
nerve for hemifacial spasm in youth. Childs Nerv Syst 2001;17:309-12.
- 22 Kobata H, Kondo A, Kinuta Y, Iwasaki K, Nishioka T, Hasegawa K, et al. Hemifacial
spasm in childhood and adolescence. Neurosurgery 1995;36:710-4.
- 23 Liang J, Guo Z, Zhang L, Yu Y. Adolescent-onset idiopathic hemifacial spasm. Neurol
India 2014;62:175-7.
- 24 Levy EI, Resnick DK, Jannetta PJ, Lovely T, Bissonette DJ. Pediatric hemifacial spasm:
The efficacy of microvascular decompression. Pediatr Neurosurg 1997;27:238-41.
- 25 Kamiguchi H, Ohira T, Ochiai M, Kawase T. Computed tomographic analysis of hemifacial
spasm: Narrowing of the posterior fossa as a possible facilitating factor for neurovascular
compression. J Neurol Neurosurg Psychiatry 1997;62:532-4.
- 26 Felício AC, de Godeiro C Jr., Borges V, de Azevedo Silva SM, Ferraz HB. Young onset
hemifacial spasm in patients with Chiari type I malformation. Parkinsonism Relat Disord
2008;14:66-8.
- 27 Mason WE, Kollros P, Jannetta PJ. Trigeminal neuralgia and its treatment in a 13-month-old
child: A review and case report. J Craniomandib Disord 1991;5:213-6.
- 28 Resnick DK, Levy EI, Jannetta PJ. Microvascular decompression for pediatric onset
trigeminal neuralgia. Neurosurgery 1998;43:804-7.
- 29 Matsushima T, Huynh-Le P, Miyazono M. Trigeminal neuralgia caused by venous compression.
Neurosurgery 2004;55:334-7.
- 30 Bahgat D, Ray DK, Raslan AM, McCartney S, Burchiel KJ. Trigeminal neuralgia in young
adults. J Neurosurg 2011;114:1306-11.
- 31 Bender MT, Pradilla G, James C, Raza S, Lim M, Carson BS, et al. Surgical treatment
of pediatric trigeminal neuralgia: Case series and review of the literature. Childs
Nerv Syst 2011;27:2123-9.
- 32 Mousavi SH, Sekula RF, Gildengers A, Gardner P, Lunsford LD. Concomitant depression
and anxiety negatively affect pain outcomes in surgically managed young patients with
trigeminal neuralgia: Long-term clinical outcome. Surg Neurol Int 2016;7:98.
- 33 Kondo A, Ishikawa J, Konishi T. The pathogenesis of hemifacial spasm: Characteristic
changes of vasculature in vertebra-basilar artery system. In: Samii M, Jannetta PJ,
editors. The Cranial Nerves: Anatomy, Pathology, Pathophysiology, Diagnosis, Treatment.
Berlin: Springer-Verlag; 1987. p. 494-501.
- 34 Pai BS, Varma RG, Kulkarni RN, Nirmala S, Manjunath LC, Rakshith S, et al. Microsurgical
anatomy of the posterior circulation. Neurol India 2007;55:31-41.
- 35 Wankhede HA, Hosmani PB, Nimje DA. Morphological study of the basilar artery in adult
human cadavers. Int J Anat Res 2014;2:497-502.
- 36 Saeki N, Rhoton AL Jr. Microsurgical anatomy of the upper basilar artery and the
posterior circle of Willis. J Neurosurg 1997;46:563-78.
- 37 Ohta M, Kobayashi M, Terano N, Wakiya K, Suzuki K, Fujimaki T, et al. Does arteriosclerosis
contribute to hemifacial spasm? Acta Neurochir (Wien) 2016;158:181-7.
- 38 Samii M, Günther T, Iaconetta G, Muehling M, Vorkapic P, Samii A, et al. Microvascular
decompression to treat hemifacial spasm: Long-term results for a consecutive series
of 143 patients. Neurosurgery 2002;50:712-8.
- 39 Han IB, Chang JH, Chang JW, Huh R, Chung SS. Unusual causes and presentations of
hemifacial spasm. Neurosurgery 2009;65:130-7.
- 40 Sindou M, Leston J, Decullier E, Chapuis F. Microvascular decompression for primary
trigeminal neuralgia: Long-term effectiveness and prognostic factors in a series of
362 consecutive patients with clear-cut neurovascular conflicts who underwent pure
decompression. J Neurosurg 2007;107:1144-53.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Gardner WJ, Miklos MV. Response of trigeminal neuralgia to decompression of sensory
root; discussion of cause of trigeminal neuralgia. J Am Med Assoc 1959;170:1773-6.
- 2 Gardner WJ, Sava GA. Hemifacial spasm: A reversible pathophysiologic state. J Neurosurg
1962;19:240-7.
- 3 Jannetta PJ. Neurovascular compression in cranial nerve and systemic disease. Ann
Surg 1980;192:518-25.
- 4 Jannetta PJ. Treatment of trigeminal neuralgia by microoperative decompression. In:
Youmans JR, editors. Neurological Surgery. 2nd ed. Vol. 6. Philadelphia, USA: W.B.
Saunders Co.; 1982. p. 3589-603.
- 5 Jannetta PJ. Microsurgical management of trigeminal neuralgia. Arch Neurol 1985;42:800.
- 6 Barba D, Alksne JF. Success of microvascular decompression with and without prior
surgical therapy for trigeminal neuralgia. J Neurosurg 1984;60:104-7.
- 7 Barker FG 2nd, Jannetta PJ, Bissonette DJ, Larkins MV, Jho HD. The long-term outcome
of microvascular decompression for trigeminal neuralgia. N Engl J Med 1996;334:1077-83.
- 8 Choi SJ, Sung KW, Sung WH, Lee JS, Kang JK, Choi CR. The clinical analysis of 75
patients which were operated on MVD. J Korean Neurosurg Soc 1990;19:506-12.
- 9 Huang CI, Chen IH, Lee LS. Microvascular decompression for hemifacial spasm: Analyses
of operative findings and results in 310 patients. Neurosurgery 1992;30:53-6.
- 10 Huh R, Han IB, Moon JY, Chang JW, Chung SS. Microvascular decompression for hemifacial
spasm: Analyses of operative complications in 1582 consecutive patients. Surg Neurol
2008;69:153-7.
- 11 Jang IH, Lee YH, Chung UW. Intraoperative electromyographic monitoring of the facial
nerve during microvascular decompression for hemifacial spasm. J Korean Acad Rehabil
Med 1994;18:142-51.
- 12 Jannetta PJ. Hemifacial spasm. Neurol Neurosurg Update Ser 1982;3:1-7.
- 13 Loeser JD, Chen J. Hemifacial spasm: Treatment by microsurgical facial nerve decompression.
Neurosurgery 1983;13:141-6.
- 14 Wilkins RH. Hemifacial spasm: A review. Surg Neurol 1991;36:251-77.
- 15 Ehni G, Woltman HW. Hemifacial spasm: Review of one hundred and six cases. Arch Neurol
Psychiatry 1945;53:205-11.
- 16 Jho HD, Jannetta PJ. Hemifacial spasm in young people treated with microvascular
decompression of the facial nerve. Neurosurgery 1987;20:767-70.
- 17 Langston JW, Tharp BR. Infantile hemifacial spasm. Arch Neurol 1976;33:302-3.
- 18 Milani N, Scaioli V, Giombini S, Grisoli M, Angelini L. Hemifacial spasm in a child.
Childs Nerv Syst 1991;7:466-8.
- 19 Jannetta PJ. Arterial compression of the trigeminal nerve at the pons in patients
with trigeminal neuralgia. J Neurosurg 1967;26 Suppl:159-62.
- 20 Feng B, Zheng X, Zhang W, Yang M, Tang Y, Zhong J, et al. Surgical treatment of pediatric
hemifacial spasm patients. Acta Neurochir (Wien) 2011;153:1031-5.
- 21 Chang JW, Chang JH, Park YG, Chung SS. Microvascular decompression of the facial
nerve for hemifacial spasm in youth. Childs Nerv Syst 2001;17:309-12.
- 22 Kobata H, Kondo A, Kinuta Y, Iwasaki K, Nishioka T, Hasegawa K, et al. Hemifacial
spasm in childhood and adolescence. Neurosurgery 1995;36:710-4.
- 23 Liang J, Guo Z, Zhang L, Yu Y. Adolescent-onset idiopathic hemifacial spasm. Neurol
India 2014;62:175-7.
- 24 Levy EI, Resnick DK, Jannetta PJ, Lovely T, Bissonette DJ. Pediatric hemifacial spasm:
The efficacy of microvascular decompression. Pediatr Neurosurg 1997;27:238-41.
- 25 Kamiguchi H, Ohira T, Ochiai M, Kawase T. Computed tomographic analysis of hemifacial
spasm: Narrowing of the posterior fossa as a possible facilitating factor for neurovascular
compression. J Neurol Neurosurg Psychiatry 1997;62:532-4.
- 26 Felício AC, de Godeiro C Jr., Borges V, de Azevedo Silva SM, Ferraz HB. Young onset
hemifacial spasm in patients with Chiari type I malformation. Parkinsonism Relat Disord
2008;14:66-8.
- 27 Mason WE, Kollros P, Jannetta PJ. Trigeminal neuralgia and its treatment in a 13-month-old
child: A review and case report. J Craniomandib Disord 1991;5:213-6.
- 28 Resnick DK, Levy EI, Jannetta PJ. Microvascular decompression for pediatric onset
trigeminal neuralgia. Neurosurgery 1998;43:804-7.
- 29 Matsushima T, Huynh-Le P, Miyazono M. Trigeminal neuralgia caused by venous compression.
Neurosurgery 2004;55:334-7.
- 30 Bahgat D, Ray DK, Raslan AM, McCartney S, Burchiel KJ. Trigeminal neuralgia in young
adults. J Neurosurg 2011;114:1306-11.
- 31 Bender MT, Pradilla G, James C, Raza S, Lim M, Carson BS, et al. Surgical treatment
of pediatric trigeminal neuralgia: Case series and review of the literature. Childs
Nerv Syst 2011;27:2123-9.
- 32 Mousavi SH, Sekula RF, Gildengers A, Gardner P, Lunsford LD. Concomitant depression
and anxiety negatively affect pain outcomes in surgically managed young patients with
trigeminal neuralgia: Long-term clinical outcome. Surg Neurol Int 2016;7:98.
- 33 Kondo A, Ishikawa J, Konishi T. The pathogenesis of hemifacial spasm: Characteristic
changes of vasculature in vertebra-basilar artery system. In: Samii M, Jannetta PJ,
editors. The Cranial Nerves: Anatomy, Pathology, Pathophysiology, Diagnosis, Treatment.
Berlin: Springer-Verlag; 1987. p. 494-501.
- 34 Pai BS, Varma RG, Kulkarni RN, Nirmala S, Manjunath LC, Rakshith S, et al. Microsurgical
anatomy of the posterior circulation. Neurol India 2007;55:31-41.
- 35 Wankhede HA, Hosmani PB, Nimje DA. Morphological study of the basilar artery in adult
human cadavers. Int J Anat Res 2014;2:497-502.
- 36 Saeki N, Rhoton AL Jr. Microsurgical anatomy of the upper basilar artery and the
posterior circle of Willis. J Neurosurg 1997;46:563-78.
- 37 Ohta M, Kobayashi M, Terano N, Wakiya K, Suzuki K, Fujimaki T, et al. Does arteriosclerosis
contribute to hemifacial spasm? Acta Neurochir (Wien) 2016;158:181-7.
- 38 Samii M, Günther T, Iaconetta G, Muehling M, Vorkapic P, Samii A, et al. Microvascular
decompression to treat hemifacial spasm: Long-term results for a consecutive series
of 143 patients. Neurosurgery 2002;50:712-8.
- 39 Han IB, Chang JH, Chang JW, Huh R, Chung SS. Unusual causes and presentations of
hemifacial spasm. Neurosurgery 2009;65:130-7.
- 40 Sindou M, Leston J, Decullier E, Chapuis F. Microvascular decompression for primary
trigeminal neuralgia: Long-term effectiveness and prognostic factors in a series of
362 consecutive patients with clear-cut neurovascular conflicts who underwent pure
decompression. J Neurosurg 2007;107:1144-53.