

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_275_20
Predictors of outcome following interventions for ruptured intracranial aneurysms in an emerging health institution in West Bengal: A 6-year experience
Authors

Background: Microsurgical clipping and endovascular coiling have remained over the past half-century, the main options for definitive treatment of ruptured intracranial aneurysms. However, recent advances in endovascular techniques have broadened their application stimulating much debate regarding the usefulness of microsurgical options. For locations with limited capacity or evolving endovascular service, however, microsurgical treatment offers not only cost-effective and durable options but also oftentimes the only option available for most patients. Materials and Methods: This was a single institution questionnaire-based retrospective study from West Bengal India. It was performed on patients with aneurysmal rupture managed from June 2010 to October 2016. Data analysis was performed with SPSS for Windows, version 21. Results: One hundred and ten patients were studied. The mean age was 50.8 years (standard deviation [SD] ±13.5) for females and 50.2 (SD ± 12.4) for males (P = 0.8112, t-test). Ninety (81.8%) patients received microsurgical clipping. Microsurgical options such as wrapping, bypass, and excision were performed for 9 (8.2%) patients. Coiling was performed for 11 (10%) patients. ACOM was the most common site for ruptured aneurysm. Ictus-intervention interval (χ2 = 10.034, P = 0.007) and multiple surgical procedures (χ2 = 8.9341, P = 0.003) were the significant outcome determinants. Overall, 72.7% of those treated had a good outcome (Glasgow Outcome Score of 4 and 5). The good outcome was higher among microsurgery groups (73.7%) compared to the coiling group (63.6%) but this difference did not achieve statistical significance (χ2 = 0.46 P = 0.4976). Conclusion: Microsurgical options achieved good outcomes in the management of ruptured aneurysms in our series. Their availability makes them first-line options for low-income settings.
Introduction
The historical landmarks in the evolution of brain aneurysm treatment from antiquity to the modern era which was heralded by the first aneurysm “clipping” by Dandy on March 23, 1937, and subsequently, the birth of endovascular coiling in 1990 by Guido Guglielmi have been well chronicled by Peschillo et al.[[1]] The pooled incidence of aneurysmal subarachnoid hemorrhage (aSAH) was 7.8 per 100,000 person-years and has remained stable.[[2]] Today, most patients with good grade aneurysmal ruptures are managed by clipping or coiling. Improved survival even among poor grade patients is increasingly reported in recent times.[[3]] The Barrow Ruptured Aneurysm Trial concluded that obliteration rates were significantly lower and re-treatment rates significantly higher among the patients undergoing coiling when compared with those undergoing clipping even though outcomes for posterior circulation favor coiling.[[4]] Although the principles and applications of microsurgical clipping remain the same to a large extent, other useful maneuvers such as wrapping, bypass, temporary occlusion of vessels, and adenosine-induced cardiac arrest may on some occasions prove helpful in the microsurgical treatment of ruptured aneurysms, thereby helping to broaden the scope and success of microsurgery.[[5]],[[6]],[[7]],[[8]]
As the global treatment paradigm for aneurysmal SAH in contemporary practice continues to lean heavily toward endovascular techniques, a continuous appraisal of surgical options in relation to the overall socioeconomic and geopolitical profiles of practice settings is required. This will help prioritize the accessibility of cost-effective and durable options to all populations especially those from developing countries and low-income settings. Such an appraisal will require scientific evidence obtained from various settings across the global socioeconomic spectrum. This study provides such an evaluation from an emerging neurosurgical center treating patients with ruptured brain aneurysms in a developing country.
Materials and Methods
An institution-based retrospective analysis of patients with aSAH managed by the neurosurgery department of Medica Institute of Neurological Diseases, Kolkata, West Bengal in India was conducted between June 2010 and November 2016. Clinical records from operation theatre logbooks, and integrated computerized hospital database system were searched. With the aid of a questionnaire, data on demographic and clinical profiles, radiologic findings, and management modalities were extracted.
Our neuroimaging protocol for the evaluation and diagnosis of suspected ruptured aneurysm included a plain cranial computerized tomography (CT) scan, CT angiography, digital subtraction angiography (DSA), and in some cases magnetic resonance imaging/magnetic resonance angiography. Choice of treatment was based on aSAH grade, location, and size of the aneurysm, comorbidities, and choice of caregivers. Doppler was used intraoperatively to assess the flow patency of vessels post clipping as well as verify the exclusion of clipped aneurysm from the brain circulation. Most patients were treated microsurgically, while patients with poor the World Federation of Neurosurgical Societies grade and comorbidity were treated with coiling. CT Angiography and DSA were performed postoperatively to assess postoperative complications such as vasospasm, brain ischemia, and cerebrospinal fluid (CSF) complications.
Inclusion criteria
Patients with ruptured intracranial aneurysm who received microsurgical treatment or endovascular intervention were selected for our study.
Data analysis
Data analysis was performed using SPSS for Windows, Chicago Illinois, USA, version 21. P < 0.05 was considered statistically significant.
Results
Patient characteristics
One hundred and ten patients who satisfied our study criteria were managed during our study period., 62 (56.4%) were female and 48 (43.6%) were male. Their ages ranged between 14 and 76 years (Mean 50.5 ± 13.0). The mean age was 50.8 ± 13.5 years) among females and 50.2 ± 12.4 years among males. The mean ages did not vary significantly between males and females (P = 0.8112, t-test). The mean ages for microsurgical and coiling groups were 51.1 ± 12.5 and 45.5 ± 16.3 years, respectively. The mean duration from ictus to presentation was 8.96 days ± 11.5 with a range of 1–69 days. The duration of hospital admission varied from 3 days to 96 days (Mean 17.6 ± 14.3). Coiled patients had an in-hospital admission period of 5–76 days (18.7 ± 21.2), while the duration varied from 3 to 96 days (17.5 ± 13.5) for the microsurgery group.
Characteristics of the aneurysms
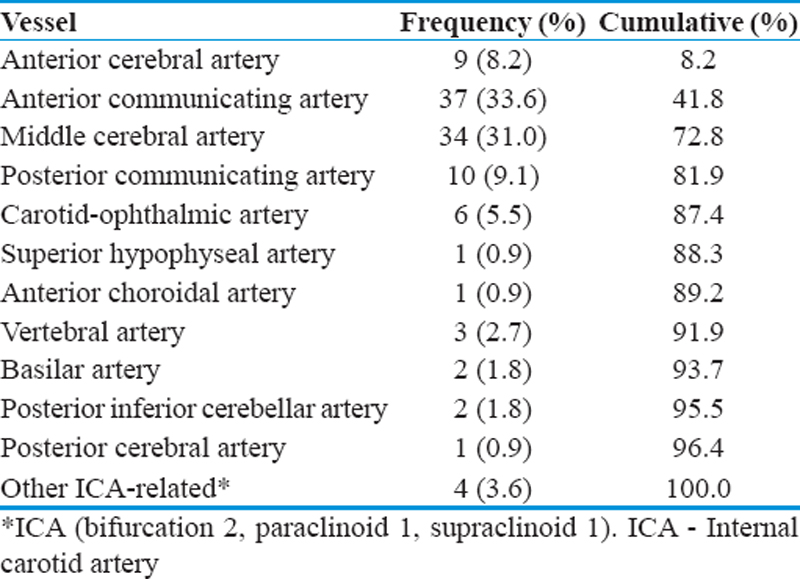
Aneurysms were saccular in 51% of cases, fusiform in 20.4%, dissecting in 10.2% cases, mycotic in 6.1% of cases, and in 12.3% of cases, the aneurysm was multiform. Ruptured anterior communicating artery (ACOM) aneurysms presented in 37 (33.6%) cases and represent the most common in our series followed by middle cerebral artery (MCA) aneurysms 34 (31.0%), and posterior communicating artery aneurysms 10 (9.1%) [[Table 1]]. Most MCA aneurysms occurred at the bifurcation in 27 (79.4%) cases.
Posterior circulation aneurysms accounted for 45.5% of coiled cases and 3.0% of microsurgical cases (P < 0.00001, χ2 = 8.9341).
Multiple aneurysms
Thirty-three aneurysms occurred as multiple aneurysms with 13 of them ruptured. Seven (53.8%) were female and 6 (46.2%) were male. MCA in 9 (27.3%) cases was the most common location affected in a setting of multiple aneurysms. However, (ACOM) in 5 (35.7%) cases was the most common identified rupture site among those with multiple aneurysms with a rupture rate of 83.3% [[Table 2]].

In 7 (53.8%) cases, two aneurysms were treated successfully at a single sitting, whereas in 5 (38.5%) patients, only the ruptured aneurysm was treated. One (1) patient with two aneurysms had two separate surgical procedures.
Treatment modalities
Microsurgical clipping was performed in 90 (81.8%) patients. Other microsurgical techniques such as wrapping, bypass, and aneurysm excision were performed in 9 (8.2%) patients. Coiling was the treatment procedure in 11 (10%) patients [[Figure 1]].

Morbidity
An additional surgical procedure was required in 43 patients (34.5%) with cranioplasty being the most common procedure (n = 13). Among this category of patients, forty of them were in the microsurgery subgroup (40.4% of microsurgery). Additional procedures include tracheostomy (11), Ventriculoperitoneal shunt (9), lumbar drain (5), external ventricular drain (1), craniectomy (1), Postoperative hematoma evacuation (1), and combination of procedures (2).
Vasospasm/cerebral ischemia was the most common complication after treatment (36.4%) and it was seen in higher proportion of coiled patients [[Table 3]]. CSF-related complications include hydrocephalus (n = 13), pseudomeningocele (4), and CSF leak (1). Hydrocephalus was the only CSF-related complication in the coiling group and occurred at a higher rate [[Figure 2]].


Cost of treatment
The mean cost of treatment for microsurgery was $10,000.00 ± 127.50, while that of coiling was $12,000 ± 277.95.
Outcome
Overall, 72.7% of patients treated had a good outcome (Glasgow Outcome Score [GOS] 4 and 5). The good outcome was higher among microsurgery groups (73.7%) compared to the coiling group (63.6%) but this difference did not achieve statistical significance (χ2 = 0.46 P = 0.4976) [[Table 4]].

Patients within the age range 41–60 years showed the best GOS [[Figure 3]]. However, there was no significant difference in the mean age between patients with poor and good GOS (t = 0.367, P = 0.714).

The mortality rate among the microsurgery group (n = 99) was 7.1% (7 patients). No mortality was recorded at discharge in the coiling group.
Discussions
The mean age in this series of ruptured aneurysm was 50.5 ± 13.0 years. There was no significant difference in age at presentation between sexes although patients treated with microsurgery appeared to be younger. However, a female preponderance was observed for both single and multiple aneurysms. This correlates with findings from previous international studies on the subject.[[2]],[[9]] Differences between the two treatment subgroups were noted with the coiling group having longer time to presentation, longer duration of admission, and lower GCS on admission [[Table 5]]. Delayed presentation highlighting poor access to care was observed among most patients in our series with a mean ictus presentation interval of 9 days. Although only a third of our patients presented within 48 h of ictus, however, delayed ictus-intervention interval was associated with better outcome (P = 0.007). However, as we did not include those who died before intervention into our study, the association between delayed ictus-intervention interval and better outcome from our study appears misleading and may not represent the true relationship between time to intervention and outcome following interventions in patients with aSAH. Sharma et al. have previously reported worse outcomes among patients with multiple intracranial aneurysms who presented early.[[10]] Therefore, with majority of our patients presenting late, we believe they represent survivors of the early phase and are probably within the rupture-rerupture time window. We believe many more patients with ruptured aneurysms may have died before having access to specialist care and natural selection has occurred in the prehospital phase. Hence, while in-hospital outcome remains good overall it can only depict the success of neurosurgical intervention, and not necessarily the true picture of the overall survival profile of ruptured intracranial aneurysms in our setting.

Saccular aneurysms were found in half of the patients making them the most common aneurysms similar to reports from other parts of the world.[[11]],[[12]] ACOM aneurysms and MCA aneurysms were the most common aneurysms among cohorts [[Table 1]]. Beck et al. had earlier reported in a German population that aneurysms at the anterior cerebral or anterior communicating arteries were significantly more likely to present with rupture, whereas MCA aneurysms were more often unruptured.[[12]] Most MCA aneurysms were located at the MCA bifurcation in 79.4 cases.
The incidence of multiple aneurysms was 11.8% in our series and this is within the range of 2%–34.5% reported by Ogeng'o et al.[[13]] Unlike the pattern of presentation among solitary aneurysmal rupture where ACOM predominates both in the prevalence of aneurysm as well as frequency of rupture, MCA aneurysms are the most prevalent in patients with multiple aneurysms. However even among those with multiple aneurysms, ACOM was still the most common rupture site observed [[Table 2]]. Our finding is in agreement with the work by Sharma et al. which reported a rupture rate of 78.6% for ACOM aneurysms.[[10]] Although the reported prevalence of aneurysmal sites varies among reports, the higher rupture rate of ACOM aneurysms in comparison to aneurysms found in other locations appears unanimous and also statistically significant.[[14]],[[15]] The rupture rate for ACOM in a setting of multiple aneurysm from our index study was 88.3% [[Table 2]]. This high associated rupture profile justifies, in our opinion, the decision to surgically treat an unruptured ACOM aneurysm coexisting with a ruptured aneurysm in another location. We believe that successful treatment of one aneurysm in a setting of multiple lesions may predispose adjacent aneurysm (s) to more precarious pressure loading raising their rupture risk. This is even more likely for ACOM aneurysms, which are associated with high de novo rupture risk. In 53.8% of our patients, two aneurysms were successfully treated at a single sitting. The number of aneurysms (multiple versus single) did not influence the outcome of treatment in our series [[Table 4]]. A similar finding has also been previously reported in an Indian setting.[[10]] This might be due to the fact that even in a setting of multiple aneurysms, only one rupture site was identified among each of our patients thereby creating equipoise between the outcome profile associated with multiple lesions and those of single ruptured aneurysms.
Microsurgical techniques as a group remain the most common treatment modality for aneurysms among our patients with clipping representing the poster child of the spectrum. In general, treatment modality for each case is selected based on aneurysm location, patient's neurological condition, and most notably affordability in our setting. We favor coiling in aneurysms of the posterior circulation. Despite the undisputed benefits of endovascular coiling, affordability remains an issue when patients are counseled in our practice setting. Our experience has been corroborated by a report showing a high cost of endovascular treatment in Morocco and aligns with the current practice trends in India.[[16]],[[17]] From our study, we found endovascular treatment more costly when compared to microsurgical treatment [[Table 5]]. Difficulties could be encountered during microsurgery requiring additional techniques. Adenosine-induced flow arrest, when used with proper caution, could be a useful and life-saving modality facilitating clip application in the event of intraoperative rupture. The experience of some of the authors of this study with adenosine-induced flow arrest in two aneurysms has been reported in the literature.[[18]] Other authors find it beneficial even for unruptured aneurysms. In three patients, we used the clip-wrap technique for giant aneurysms where clipping application alone was inadequate. All the patients who had these additional microsurgical maneuvers experienced good outcomes.[[5]] Figueiredo et al. reported nine cases of otherwise unclippable aneurysms which they managed successfully using the clip-wrap technique and concluded that it was safe and could be associated with a low rate of acute or delayed postoperative complications.[[6]] More recently, a large series of thirty patients with both ruptured and unruptured aneurysms managed with Gore-Tex clip-wrap technique with good results has been reported.[[19]] Another useful microsurgical technique, we successfully applied in the treatment of two patients in our series with complex aneurysms was the vessel bypass technique. We also had good outcome with this technique. The usefulness of vascular bypass in managing aneurysms with complex morphology has also been reported previously.[[20]]
Overall, 40.4% (40) of patients who had microsurgery required additional procedures with cranioplasty being the most common (13.1%). Among complications experienced by patients, [[Figure 2]] intraoperative rupture was not observed among coiled aneurysms in our series. Furthermore, the only CSF-related complication observed among coiled aneurysms in our series was hydrocephalus in 1 patient (10%), whereas, pseudomeningoceles and cerebrospinal fluid leaks were more commonly observed among the microsurgery subgroup. Furthermore, multiple surgical procedures were found to be an important determinant of outcome (P = 0.003). A good outcome (GOS 4 and 5) was observed at discharge in patients who had microsurgical intervention (73.7%). Although 73.7 percent of patients in the microsurgery group compared to 63.6% among the coiling group achieved good outcome, this difference was not statistically significant. Therefore on the basis of our study, we found no significant difference in relation to overall outcome between microsurgery and coiling, χ2 = 0.46, P = 0.4976. However, we are careful not to make categorical conclusions since the sample size for the coiling subgroup was much less and the sampling frame was not uniform. While some authors have reported better outcomes with endovascular coiling as they continue to gain ascendancy over microsurgical techniques in many locations globally, others report no statistical difference in outcome and suggested that both methods should be considered as complementary to one another.[[10]],[[21]],[[22]] Within the limits of the power of our study, we believe that availability of microsurgical techniques will most likely make these techniques the mainstay of treatment for ruptured intracranial aneurysms in low-income settings such as ours in the foreseeable future. Although the mean cost of clipping appeared lower than coiling, we did not compare the cost-effectiveness profiles of both procedures. Coiling and other endovascular procedures although gaining predominance globally, especially in the developed world will likely complement microsurgery for the treatment of aneurysms located in remote intracranial sites such as the posterior circulation. Endovascular options will also play an important role in cases where aneurysm anatomy or patients status render microsurgery hazardous.
Limitations
Although we compared the length of hospital admission between the two subgroups, we could not retrieve from our records, the length of intensive care unit admission for the coiling group. We believe this is a limitation because we could not compare this profile among the treatment subgroups and hope to address this in a future prospective study. We also could not evaluate the profile of residual aneurysms and their follow-up treatment.
Conclusion
Ruptured intracranial aneurysm presenting singly or as multiple lesion occur more common among females with the highest rupture rate reported among ACOM aneurysms. Microsurgical techniques have been rewarded with good outcomes in our experience. We believe the availability, low relative cost, and associated good outcomes for microsurgical options combine to make them choice options for our environment. Our experience may be helpful to other developing countries, especially those locations where coiling is not yet readily available. We however consider microsurgery and endovascular coiling as a complementary pair of beneficial options rather than irreconcilable opponents competing for mastery in the intracranial vascular ring. Our study is limited by the small number of patients who had endovascular coiling.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Peschillo S, Caporlingua A, Caporlingua F, Guglielmi G, Delfini R. Historical landmarks in the management of aneurysms and arteriovenous malformations of the central nervous system. World Neurosurg 2016;88:661-71.
- 2 Linn FH, Rinkel GJ, Algra A, van Gijn J. Incidence of subarachnoid hemorrhage: Role of region, year, and rate of computed tomography: A meta-analysis. Stroke 1996;27:625-9.
- 3 Howard BM, Barrow DL. Outcomes for patients with poor-grade subarachnoid hemorrhage: To treat or not to treat? World Neurosurg 2016;86:30-2.
- 4 Spetzler RF, McDougall CG, Zabramski JM, Albuquerque FC, Hills NK, Russin JJ, et al. The barrow ruptured aneurysm trial: 6-year results. J Neurosurg 2015;123:609-17.
- 5 Andrade-Barazarte H, Luostarinen T, Goehre F, Kivelev J, Jahromi BR, Ludtka C, et al. Transient cardiac arrest induced by adenosine: A tool for contralateral clipping of internal carotid artery-ophthalmic segment aneurysms. World Neurosurg 2015;84:1933-40.
- 6 Figueiredo EG, Foroni L, Monaco BA, Gomes MQ, Sterman Neto H, Teixeira MJ. The clip-wrap technique in the treatment of intracranial unclippable aneurysms. Arq Neuropsiquiatr 2010;68:115-8.
- 7 Fraser JF, Stieg PE. Surgical bypass for intracranial aneurysms: Navigating around a changing paradigm. World Neurosurg 2011;75:414-7.
- 8 Griessenauer CJ, Poston TL, Shoja MM, Mortazavi MM, Falola M, Tubbs RS, et al. The impact of temporary artery occlusion during intracranial aneurysm surgery on long-term clinical outcome: Part I. Patients with subarachnoid hemorrhage. World Neurosurg 2014;82:140-8.
- 9 Froelich JJ, Neilson S, Peters-Wilke J, Dubey A, Thani N, Erasmus A, et al. Size and location of ruptured intracranial aneurysms: A 5-year clinical survey. World Neurosurg 2016;91:260-5.
- 10 Sharma P, Mehrotra A, Das KK, Bhaisora KS, Sardhara J, Godbole CA, et al. Factors predicting poor outcome in a surgically managed series of multiple intracranial aneurysms. World Neurosurg 2016;90:29-37.
- 11 Nabaweesi-Batuka J, Kitunguu PK, Kiboi JG. Pattern of cerebral aneurysms in a Kenyan population as seen at an Urban hospital. World Neurosurg 2016;87:255-65.
- 12 Beck J, Rohde S, Berkefeld J, Seifert V, Raabe A. Size and location of ruptured and unruptured intracranial aneurysms measured by 3-dimensional rotational angiography. Surg Neurol 2006;65:18-25.
- 13 Ogeng'o JA, Otieno BO, Kilonzi J, Sinkeet SR, Muthoka JM. Intracranial aneurysms in an African country. Neurol India 2009;57:613-6.
- 14 Lu HT, Tan HQ, Gu BX, Wu-Wang , Li MH. Risk factors for multiple intracranial aneurysms rupture: A retrospective study. Clin Neurol Neurosurg 2013;115:690-4.
- 15 Nehls DG, Flom RA, Carter LP, Spetzler RF. Multiple intracranial aneurysms: Determining the site of rupture. J Neurosurg 1985;63:342-8.
- 16 Ambekar S, Madhugiri V, Pandey P, Yavagal DR. Cerebral aneurysm treatment in India: Results of a national survey regarding practice patterns in India. Neurol India 2016;64 Suppl: S62-9.
- 17 Amine C, Najia EA, Hatim I, Adil A, Yahya C, Abdeljalil EQ. The cost of management of intracranial aneurysms by embolization in morocco: About 48 cases. Int J Pharm Pharm Sci 2014;6 Suppl 2:822-6.
- 18 Deb K, Ghosh J, Jain H, Tripathy LN. Adenosine in difficult aneurysm surgeries: Report of two cases. J Neuroanaesth Crit Care 2014;1:66-8.
- 19 Safavi-Abbasi S, Moron F, Sun H, Wilson C, Frock B, Oppenlander ME, et al. Techniques and outcomes of gore-tex clip-wrapping of ruptured and unruptured cerebral aneurysms. World Neurosurg 2016;90:281-90.
- 20 Tian Y, Zhu W, Mao Y. Surgical strategies for treatment of complex anterior cerebral artery aneurysms. World Neurosurg 2014;81:304-5.
- 21 Gupta MM, Bithal PK, Dash HH, Chaturvedi A, Prabhakar H. Clinical outcome of intracranial aneurysms: A retrospective comparison between endovascular coiling and neurosurgical clipping. Indian J Anaesth 2008;52:63.
- 22 Zanaty M, Chalouhi N, Starke RM, Daou B, Todd M, Bayman E, et al. Short-term outcome of clipping versus coiling of ruptured intracranial aneurysms treated by dual-trained cerebrovascular surgeon: Single-institution experience. World Neurosurg 2016;95:262-9.
Address for correspondence
Publication History
Received: 06 June 2020
Accepted: 08 February 2021
Article published online:
16 August 2022
© 2021. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Peschillo S, Caporlingua A, Caporlingua F, Guglielmi G, Delfini R. Historical landmarks in the management of aneurysms and arteriovenous malformations of the central nervous system. World Neurosurg 2016;88:661-71.
- 2 Linn FH, Rinkel GJ, Algra A, van Gijn J. Incidence of subarachnoid hemorrhage: Role of region, year, and rate of computed tomography: A meta-analysis. Stroke 1996;27:625-9.
- 3 Howard BM, Barrow DL. Outcomes for patients with poor-grade subarachnoid hemorrhage: To treat or not to treat? World Neurosurg 2016;86:30-2.
- 4 Spetzler RF, McDougall CG, Zabramski JM, Albuquerque FC, Hills NK, Russin JJ, et al. The barrow ruptured aneurysm trial: 6-year results. J Neurosurg 2015;123:609-17.
- 5 Andrade-Barazarte H, Luostarinen T, Goehre F, Kivelev J, Jahromi BR, Ludtka C, et al. Transient cardiac arrest induced by adenosine: A tool for contralateral clipping of internal carotid artery-ophthalmic segment aneurysms. World Neurosurg 2015;84:1933-40.
- 6 Figueiredo EG, Foroni L, Monaco BA, Gomes MQ, Sterman Neto H, Teixeira MJ. The clip-wrap technique in the treatment of intracranial unclippable aneurysms. Arq Neuropsiquiatr 2010;68:115-8.
- 7 Fraser JF, Stieg PE. Surgical bypass for intracranial aneurysms: Navigating around a changing paradigm. World Neurosurg 2011;75:414-7.
- 8 Griessenauer CJ, Poston TL, Shoja MM, Mortazavi MM, Falola M, Tubbs RS, et al. The impact of temporary artery occlusion during intracranial aneurysm surgery on long-term clinical outcome: Part I. Patients with subarachnoid hemorrhage. World Neurosurg 2014;82:140-8.
- 9 Froelich JJ, Neilson S, Peters-Wilke J, Dubey A, Thani N, Erasmus A, et al. Size and location of ruptured intracranial aneurysms: A 5-year clinical survey. World Neurosurg 2016;91:260-5.
- 10 Sharma P, Mehrotra A, Das KK, Bhaisora KS, Sardhara J, Godbole CA, et al. Factors predicting poor outcome in a surgically managed series of multiple intracranial aneurysms. World Neurosurg 2016;90:29-37.
- 11 Nabaweesi-Batuka J, Kitunguu PK, Kiboi JG. Pattern of cerebral aneurysms in a Kenyan population as seen at an Urban hospital. World Neurosurg 2016;87:255-65.
- 12 Beck J, Rohde S, Berkefeld J, Seifert V, Raabe A. Size and location of ruptured and unruptured intracranial aneurysms measured by 3-dimensional rotational angiography. Surg Neurol 2006;65:18-25.
- 13 Ogeng'o JA, Otieno BO, Kilonzi J, Sinkeet SR, Muthoka JM. Intracranial aneurysms in an African country. Neurol India 2009;57:613-6.
- 14 Lu HT, Tan HQ, Gu BX, Wu-Wang , Li MH. Risk factors for multiple intracranial aneurysms rupture: A retrospective study. Clin Neurol Neurosurg 2013;115:690-4.
- 15 Nehls DG, Flom RA, Carter LP, Spetzler RF. Multiple intracranial aneurysms: Determining the site of rupture. J Neurosurg 1985;63:342-8.
- 16 Ambekar S, Madhugiri V, Pandey P, Yavagal DR. Cerebral aneurysm treatment in India: Results of a national survey regarding practice patterns in India. Neurol India 2016;64 Suppl: S62-9.
- 17 Amine C, Najia EA, Hatim I, Adil A, Yahya C, Abdeljalil EQ. The cost of management of intracranial aneurysms by embolization in morocco: About 48 cases. Int J Pharm Pharm Sci 2014;6 Suppl 2:822-6.
- 18 Deb K, Ghosh J, Jain H, Tripathy LN. Adenosine in difficult aneurysm surgeries: Report of two cases. J Neuroanaesth Crit Care 2014;1:66-8.
- 19 Safavi-Abbasi S, Moron F, Sun H, Wilson C, Frock B, Oppenlander ME, et al. Techniques and outcomes of gore-tex clip-wrapping of ruptured and unruptured cerebral aneurysms. World Neurosurg 2016;90:281-90.
- 20 Tian Y, Zhu W, Mao Y. Surgical strategies for treatment of complex anterior cerebral artery aneurysms. World Neurosurg 2014;81:304-5.
- 21 Gupta MM, Bithal PK, Dash HH, Chaturvedi A, Prabhakar H. Clinical outcome of intracranial aneurysms: A retrospective comparison between endovascular coiling and neurosurgical clipping. Indian J Anaesth 2008;52:63.
- 22 Zanaty M, Chalouhi N, Starke RM, Daou B, Todd M, Bayman E, et al. Short-term outcome of clipping versus coiling of ruptured intracranial aneurysms treated by dual-trained cerebrovascular surgeon: Single-institution experience. World Neurosurg 2016;95:262-9.