
Subscribe to RSS
DOI: 10.12945/j.aorta.2013.13.005
A Circular Surgical Stapler Designed to Anastomose Aorta and Dacron Tube Graft
Validation of the Concept and Comparison to Hand-Sewn Anastomosis in Bench ExperimentsCorresponding Author
Publication History
16 January 2013
13 February 2013
Publication Date:
28 September 2018 (online)
Abstract
Background: A circular aortic stapler has been developed to anastomose the open end of the aorta to a size-matched Dacron tube graft in one quick motion and without having to pull sutures through the aortic wall.
Methods: A prototype was developed, and its design and function were tested in bench experiments and compared with hand-sewn anastomosis. The basic design of the stapler is a central rod (anvil) surrounded by 10 stapling limbs, which can be closed over the anvil in a full circle, with staples extruded by turning a knob at the back. To test its function, a Dacron tube graft was inserted in the middle of a length of bovine aorta. One side was anastomosed with the stapler and the other hand-sewn in each of 10 experiments. Bovine blood was infused under increasing pressure.
Results: It took considerably less time to complete the stapled anastomosis than the hand-sewn side (3 minutes, 46 seconds versus 15 minutes, 42 seconds). Initial leak occurred at low pressures on the hand-sewn side (mean pressure 40 mm Hg) compared with the stapled side (mean pressure 70 mm Hg). In 7 of 10 experiments, the leak became too brisk on the hand-sewn side to sustain pressure, compared with 3 of 10 with stapled anastomoses. The stapling device performed well in all cases except when the bovine aorta was too thick for the staples (two cases) or when there was a missed branch at the anastomotic site (one case).
Conclusions: These experiments validate the concept and the design of this aortic stapler. There are some limitations in the current design, which will need to be modified before its use in live animals or clinically.
#
Introduction
Surgery for ascending aortic replacement continues to be challenging, particularly in cases of acute type A aortic dissection. The risk of mortality remains high[1] [2], and postoperative bleeding is a frequent complication[3], even with many recent advances in aortic surgery[4] [5]. To reduce the time it takes to replace the torn aorta with a Dacron graft and to prevent postoperative bleeding from needle holes, a surgical stapler has been designed to perform this task efficiently, expeditiously, and without the need to pull sutures through diseased aorta. A prototype of the stapler was developed (Synectic Engineering, Milford, CT) and a set of bench experiments performed to validate its effectiveness, as well as to compare it to hand-sewn anastomosis between bovine aorta and a size-matched Dacron graft. The present report describes the design of the circular aortic stapler and the results of the validation experiments performed.
#
Methods
Description of the Stapler
The stapler is designed with a central rod (anvil), which in the current prototype is made to accept a 30-mm Dacron graft snugly over it. There are 10 stapling limbs, which are situated around the anvil in a complete circle. These can open widely or close over the anvil with the twisting of a knob at the back of the instrument. Each limb has three titanium staples, in two rows, which will fully form to tightly hold together an aorta up to 4–6-mm in thickness and the Dacron graft ([Fig. 1]).

Function of the Stapler
The Dacron graft (30 mm for this prototype) is sleeved over the anvil, so that the edge of the graft matches the edge of the anvil. A #0 silk tie is placed around the Dacron graft over the anvil and tied to secure the graft in place ([Fig. 2]). [Figure 3] shows aortic dissection type A, with the portion containing the intimal tear excised. The proximal cut end of the aorta is held open, and the stapler's anvil with the Dacron graft sleeved over it is inserted into the aorta approximately 1–1.5 cm deep. A strip of Dacron can be placed around the aorta for further reinforcement of the anastomosis. The rear knob is turned clockwise to close the stapling limbs over the graft and the anvil ([Fig. 4]). Once closed, further turning the knob will extrude the staples from the stapling limbs into the aorta and the Dacron graft and then turn the ends against the anvil to form their final shape. This results in applying 2 rows of 15 staples each around the entire circumference of the aorta and thus completes an airtight anastomosis ([Fig. 5]). The stapling limbs are reopened by turning the knob counterclockwise. The #0 silk tie is cut and removed, and the anastomosed graft and aorta are gently teased to free up and remove the stapler ([Fig. 6]).





#
Validating Experiments
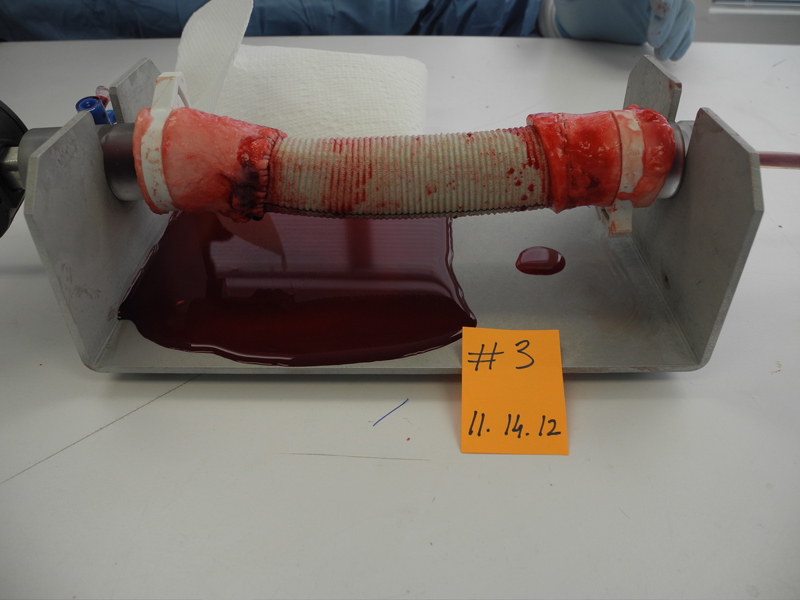
An apparatus was constructed on which a bovine aorta could be mounted lengthwise with both ends closed. It was then infused with fluids or blood from one end, and a pressure manometer was connected to the other end. Bovine aortas were obtained from a supplier in Texas along with citrate-phosphate-dextrose (CPD)-preserved bovine blood. A portion of the bovine aorta, usually proximal descending aorta, approximately 20 cm in length and with a diameter of 30 mm, was mounted on the apparatus. Branches were sought and ligated with sutures. The aorta was then divided in the middle, and a 10–15-cm-long segment of 30-mm Dacron graft was interposed, which required 2 aorta-graft anastomoses. In each of the experiments, one side was anastomosed with the circular stapler and the other was hand-sewn with a 3–0 polypropylene running suture. The entire aorta-graft segment was then filled with bovine blood, with care taken to ensure all air was expelled. Blood was then infused with a pump, and pressure in the aorta-graft segment was increased. [Figure 7] shows results from experiment 2, with a pool of blood leaking from the hand-sewn side and only a few drops leaking from the stapled anastomosis. [Figure 8] shows similar results from experiment 3.

The following data were recorded for each experiment: (1) length of time (in minutes) it took to complete the stapled versus the hand-sewn anastomosis; (2) the pressure at which the first leak occurred in either of the anastomoses; and (3) the pressure at which the leak became large enough, from either anastomosis, so that the pressure in the aorta could not be raised any further. For the stapler, we also made observations to answer the following questions: (1) Did the stapler perform as it was designed to? (2) Would there be modifications required before the stapler could be used clinically?
#
#
#
Results
The time to perform the stapled anastomosis ranged from 1 minute, 46 seconds to 4 minutes, 30 seconds (mean 3 minutes, 45 seconds). For the hand-sewn anastomosis, it ranged from 11 minutes, 13 seconds to 20 minutes, 40 seconds (mean 15 minutes, 42 seconds; [Table 1]).
|
Experiment |
Time to complete stapled anastomosis |
Time to complete hand-sewn anastomosis |
|---|---|---|
|
1 |
3 min 50 s |
16 min |
|
2 |
[*] |
16 min |
|
3 |
4 min 20 s |
13 min |
|
4 |
[*] |
13 min 30 s |
|
5 |
3 min 45 s |
19 min 20 s |
|
6 |
4 min 23 s |
20 min 40 s |
|
7 |
4 min |
11 min 13 s |
|
8 |
4 min 30 s |
16 min 8 s |
|
9 |
1 min 46 s |
12 min 44 s |
|
10 |
3 min 27 s |
17 min 12 s |
|
Mean |
3 min 45 s |
15 min 42 s |
This table lists the time to perform each of the 10 stapled and 10 hand-sewn anastomoses. In two of the stapled anastomoses, the time was not recorded. Note the significantly shorter time for the stapled anastomoses.
* Not recorded.
The pressure at which any leak appeared in the stapled anastomosis ranged from 36–135 mm Hg (mean pressure 76.5 mm Hg), and on the hand-sewn side, it ranged from 10–106 mm Hg (mean 40.6 mm Hg; [Table 2]). In 5 of the 10 hand-sewn anastomoses, the initial leak occurred at a pressure of <13 mm Hg.
The pressure at which the initial leak appeared is recorded for stapled and hand-sewn anastomoses for all 10 experiments. Note that in 8 of the 10 experiments, the leak appeared at much lower pressures on the hand-sewn side. In one, it was at the same pressure, and in another, the stapled anastomosis leaked first.
In 7 of the 10 experiments, the leak from the hand-sewn side became so brisk that pressure could not be raised further. The pressure ranged from 40–98 mm Hg (mean 70 mm Hg). In the other three experiments, the stapled side leaked briskly and caused the pressure to drop ([Table 3]). At the end of the experiments, when we examined the three stapled anastomoses that had leaked, we noted that in two of them, the bovine aorta was unevenly thick in places and measured >7 mm in thickness, where the staples were not deep enough to penetrate the full thickness, thus causing the leaks. In the third, there was a missed branch; the staples were in the middle of the branch, and the leak was caused at that point.
|
Experiment |
Stapled anastomosis |
Hand-sewn anastomosis |
|---|---|---|
|
1 |
… |
80 mm Hg |
|
2 |
… |
80 mm Hg |
|
3 |
… |
40 mm Hg |
|
4 |
… |
70 mm Hg |
|
5 |
115 mm Hg[*] |
… |
|
6 |
80 mm Hg[†] |
… |
|
7 |
73 mm Hg[*] |
… |
|
8 |
… |
50 mm Hg |
|
9 |
… |
73 mm Hg |
|
10 |
… |
98 mm Hg |
|
Total |
3 of 10 |
7 of 10 |
This table lists the pressure at which the leak became so brisk that the pressure could not be raised any further. In 7 of 10 cases, it was the hand-sewn side that leaked briskly. In three cases, the stapled side leaked briskly. The causes for the leak in these three stapled cases are listed.
* Aorta too thick, so the staples could not penetrate through the full thickness.
† Staples went through a branch that was missed.
#
Discussion
A circular stapler has been designed to anastomose the open aortic end to a size-matched Dacron tube graft. This report describes the device and validates its function during bench experiments. The bench testing showed the stapler to have functioned exactly as designed and intended. It reduced the time to perform the anastomosis significantly compared with the hand-sewn side. Also, in the seven experiments in which the bovine aorta matched the conditions as intended for the stapler, it functioned perfectly, with no leaks. The hand-sewn side started leaking at low pressures, all from needle holes, and by the time pressure was raised to 100 mm Hg, the leaks had become so brisk that the pressure could not be raised further. To the best of our knowledge, this is the first time a surgical stapler has been designed specifically for anastomosing aorta and Dacron tube graft.
Observations
We have made the following observations as a result of this study:
-
The current prototype is made to accept a 30-mm Dacron tube graft. Eventually, multiple sizes of staplers will be made to match the various sizes of Dacron tube grafts used clinically.
-
The current prototype needs to be lengthened so that when working in a deep chest, the hands and the device will be outside the chest, and only the anvil with the surrounding limbs will be lowered into the cavity. This will not alter the basic design.
-
To interpose a tube graft in, for instance, the ascending aorta, two separate Dacron grafts will have to be anastomosed with the stapler, and then the two grafts will be sewn together by hand with a running suture (this would be much easier than sewing the dissected aortic ends and will take just a few minutes).
-
This device is circular and is not usable in cases in which the aorta is biased and not circular.
The basic concept of the stapling device for anastomosing aorta to Dacron tube graft is validated.
#
#
The Editor is a “fan” of hand-sewn anastomoses, feeling that sutures placed by hand can accommodate the irregularities in the aorta (thin areas, areas of plaque or calcification) not amenable to automatic devices. However, this device–a life-long dream for Dr. Raza–appears very well thought out and well designed. We look forward to hearing more about final refinements, regulatory approvals, and progression to clinical availability.
Questions
-
When will this product become clinically available?
We will seek to commercialize through licensing of the intellectual property by working with Columbia Technology Ventures, the technology transfer office of Columbia University.
-
What are the regulatory hurdles?
We would expect that this would be a 510K device and the company that brings the device to market will need to work with regulatory agencies on the appropriate clearance.
-
Do you intend this more for dissections, or for aneurysms as well?
It was the frustrations of operating on cases of acute aortic dissections, with sutures tearing through the aorta, the long bypass run and circulatory arrest times that led to the development of this device. But of course it can be and I hope it will be used in every case of aortic surgery, where a tube graft and aorta are to be anastomosed. The experiments described in this article were performed on healthy bovine aortas.
#
-
References
- 1 Williams JB, Peterson ED, Zhao Y, O'Brien SM, Anderson ND, Miller DC. , et al. Contemporary results for proximal aortic replacement in North America. J Am Coll Cardiol 2012; 60 (13) 1156-1162
- 2 Trimarchi S, Nienaber CA, Rampoldi V, Myrmel T, Suzuki T, Mehta RH. , et al. Contemporary results of surgery in acute type A aortic dissections: The International Registry of Acute Aortic Dissection experience. J Thorac Cardiovasc Surg 2005; 129 (01) 112-122
- 3 Hoefer D, Ruttman E, Riha M, Shobersberger W, Mayr A, Laufer G, Bonatti J. Factors influencing intensive care unit length of stay after surgery for acute aortic dissection type A. Ann Thorac Surg 2002; 73 (03) 714-718
- 4 Davies RR, Coe MP, Mandapati D, Gallo A, Botta DM, Elefteriades JA, Coady MA. What is the optimal management of late-presenting survivors of acute type A aortic dissection?. Ann Thorac Surg 2007; 83 (05) 1593-1602
- 5 Svensson LG, Crawford ES, Hess KR, Coselli JS, Raskin S, Shenaq SA, Safi HJ. Deep hypothermia with circulatory arrest: Determinants of stroke and early mortality in 656 patients. J Thorac Cardiovasc Surg 1993; 106 (01) 19-28
Corresponding Author
-
References
- 1 Williams JB, Peterson ED, Zhao Y, O'Brien SM, Anderson ND, Miller DC. , et al. Contemporary results for proximal aortic replacement in North America. J Am Coll Cardiol 2012; 60 (13) 1156-1162
- 2 Trimarchi S, Nienaber CA, Rampoldi V, Myrmel T, Suzuki T, Mehta RH. , et al. Contemporary results of surgery in acute type A aortic dissections: The International Registry of Acute Aortic Dissection experience. J Thorac Cardiovasc Surg 2005; 129 (01) 112-122
- 3 Hoefer D, Ruttman E, Riha M, Shobersberger W, Mayr A, Laufer G, Bonatti J. Factors influencing intensive care unit length of stay after surgery for acute aortic dissection type A. Ann Thorac Surg 2002; 73 (03) 714-718
- 4 Davies RR, Coe MP, Mandapati D, Gallo A, Botta DM, Elefteriades JA, Coady MA. What is the optimal management of late-presenting survivors of acute type A aortic dissection?. Ann Thorac Surg 2007; 83 (05) 1593-1602
- 5 Svensson LG, Crawford ES, Hess KR, Coselli JS, Raskin S, Shenaq SA, Safi HJ. Deep hypothermia with circulatory arrest: Determinants of stroke and early mortality in 656 patients. J Thorac Cardiovasc Surg 1993; 106 (01) 19-28